
Table of Contents
Entamoeba histolytica is a parasitic protozoan that causes amebic dysentery and can lead to severe complications like liver abscesses. Common in areas with poor sanitation, it is vital to understand its symptoms, methods of diagnosis, and treatment options for effective management. By infecting the mucosa of the colon, this ameba infect people, causing flask-shaped lesions and bloody diarrhea. According to CDC, amebiasis caused by Entamoeba histolytica is one of the leading causes of parasitic deaths worldwide.
The trophozoite secretes lyticenzymes, which can spread to other tissues, including the liver, resulting in amebic ulceration. Despite the fact that E. dispar looks like E. histolytica, it is not pathogenic. The distinguishing characteristic of these two types is established when absorbed red blood cells can be seen within Entamoeba histolytica trophozoites.
Symptoms of Entamoeba histolytica
The symptoms of Entamoeba histolytica can range from mild to severe, depending on the extent of the infection:
- Mild Symptoms:
- Intermittent diarrhea
- Abdominal cramping
- Fatigue
- Severe Symptoms:
- Bloody diarrhea
- High fever
- Weight loss
- Abdominal tenderness
- Liver abscesses in advanced cases
If untreated, Entamoeba histolytica may invade other organs, causing systemic infections.
Morphology of Entamoeba
Trophozoites
The trophozoites (trophs) of E. histolytica range in size from 8 to 65 µm, with an average size of 12 to 25 µm. Please note that parasite names are often just the first letter of the genus followed by the name of the species; E. histolytica is the abbreviated version of Entamoeba histolytica.
The trophozoite shows quick, unidirectional, gradual movement with the aid of finger-like hyaline pseudopods. A small central mass of chromatin called the karyosome usually exists in the single core (also referred to as karyosomal chromatin). Karyosome variants comprise excentric or fractured karyosomal material. The Karyosom of this amebic parasite, called peripheral chromatin, is encircled by chromatin material. Usually, this peripheral chromatin is finely dispersed and uniformly around the nucleus. There may also be variations, such as unparalleled peripheral chromatin.
While the appearance of the karyosome and peripheral chromatin can differ, most trophozoites retain the more common characteristics stated. When unstained preparations are stained, the nucleus becomes visible. Lightly stained fibrils can be visible between the karyosome and peripheral chromatin in stained preparations. The cytoplasm of the E. histolytica trophozoite is finely granular and has a ground glass appearance. Since E. histolytica is the only intestinal ameba with this trait, red blood cells (RBCs) in the cytoplasm are considered diagnostic. Bacteria, yeast, and other debris can also be found in the cytoplasm, but their appearance is not indicative of a disease.
Cysts
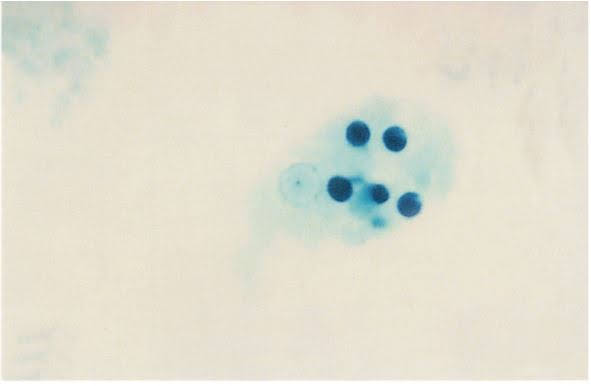
Entamoeba histolytica cysts are usually smaller than trophs, reaching 8 to 22 μm in diameter, with an average range of 12 to 18 μm. This morphologic shape can be distinguished by the appearance of a hyaline cyst wall. Young cysts typically contain unorganized chromatin content that turns into chromatoid bars, which are squared or round-ended structures that contain compact RNA material. In young cysts, a diffuse glycogen mass, a cytoplasmic region with no fixed boundaries that is thought to represent stored food, is also visible.
The glycogen mass in the cyst normally vanishes as it matures, indicating that the processed food is being used. It is common to see one to four nuclei. These nuclei resemble trophozoite nuclei in any way but size. Eccentric (rather than central) karyosomes, thin plaques of peripheral chromatin, or a crescent-shaped clump of peripheral chromatin on one side of the nucleus are some of the most frequent nuclear anomalies. The infective cyst is quadrinucleated until it reaches adulthood (containing four nuclei). The cytoplasm is fine and granular and does not alter. In the cyst phase, there are no RBCs, bacteria, yeast, or other debris.

Laboratory Diagnosis of Entamoeba histolytica
Normal and specialized approaches may be used in the laboratory diagnosis of an Entamoeba histolytica infection. Material obtained from a sigmoidoscopy operation, as well as hepatic abscess material, can be treated and analyzed in the same way as a suspicious stool sample undergoing routine examination. In culture, E. histolytica is assisted by a special medium known as TYI-S-33.
Other laboratory methods, such as immunologically based protocols, can be used where E. histolytica is suspected but not found in stool samples. Antigen analyses, enzyme-linked immunosorbent assays (ELISA), indirect hemagglutination (IHA), gel diffusion precipitin (GDP), and indirect immunofluorescence(IIF) are all currently available methods. There are serologic tests available to diagnose E. histolytica, but they are usually only useful in cases of extraintestinal infections.
Diagnosing Entamoeba histolytica involves identifying its cysts or trophozoites in stool samples. Advanced methods help confirm infections more accurately:
- Microscopy: Observing cysts in stool specimens.
- Molecular Techniques: PCR tests to differentiate between Entamoeba histolytica and non-pathogenic species like Entamoeba dispar.
- Imaging: Ultrasound or CT scans to detect liver abscesses in patients with severe symptoms.
Clinical Information
Entamoeba dispar, a nonpathogenic ameba with morphological similarities to E. histolytica, was also discovered. As a result, morphology alone is always insufficient to differentiate these two. Because of the difficulty in distinguishing between these two parasites, the laboratory sometimes reports both names when trophozoites without RBCs and/or cysts are found. If, on the other hand, trophozoites are found with ingested RBCs, they should be reported as E. histolytica. Speciation involves advanced testing methodologies such as DNA probes and electrophoresis techniques designed to identify enzymes in situations where recognition is not obvious.
Treatment Options for Entamoeba histolytica
Effective treatment depends on the stage and severity of the infection:
- Medications:
- Metronidazole: To treat invasive infections.
- Paromomycin: To clear intestinal cysts and prevent recurrence.
- Severe Cases:
- Drainage procedures for large liver abscesses.
- Hospitalization for systemic infections.
Prompt treatment reduces complications and prevents transmission to others.
Prevention of Entamoeba histolytica Infections
Preventing infections involves maintaining good hygiene and avoiding contaminated food or water:
- Boil Drinking Water: Especially in areas with poor sanitation.
- Wash Hands Regularly: Before meals and after using the toilet.
- Avoid Raw or Unwashed Produce: Properly wash or cook fruits and vegetables.
- Education in Endemic Areas: Awareness programs on parasite transmission.
Reference:
- C.P. Baveja, 2017 Medical Parasitology, 4th Edition, Arya Publications.
- WHO
- CDC