
Table of Contents
As a result of interfering factors, test results might be affected. When it comes to interference factors, it relies on the method adopted to analyze the same analyte. Hemolysis, lipemia, icterus, drugs, paraproteins, and other sample contaminants, such as gels, tube additives, and fibrin clots, are all examples of interference factors that might occur. A clinically significant interference factor is one whose bias exceeds the maximum allowed deviation for a measuring technique.
There are endogenous and exogenous interferences. Endogenous interferences come from the patient’s sample, whereas exogenous interferences come from the addition of various substances to the patient’s sample
Hemolysis
When erythrocytes and other blood cells are ruptured, they release cell components into plasma, which causes the serum (or plasma) to become red to varying degrees following centrifugation. Although hemoglobin is the most abundant protein in red blood cells, hemolysis is not always linked with the release of hemoglobin into the surrounding extracellular fluid. In vivo hemolysis and in vitro hemolysis are the two most common types of hemolysis in the body and laboratory.
Hemolysis in vivo, which happens in the body before blood is taken, is caused by a pathologic condition. It can be caused by many biochemical (enzyme deficiencies, erythrocyte membrane abnormalities, hemoglobinopathies), physical (prolonged marching, drumming, prosthetic heart valves), chemical (ethanol, drug overdose, poisons, snake venom), immunological (autoantibodies), and infectious causes (babesiosis, malaria). According on the location of the breakdown of red blood cells, in vivo hemolysis can be further divided into intravascular and extravascular hemolysis. Internal hemolysis is a direct and rapid disruption of red blood cells as a result of vasculature cell injury, whereas extravascular hemolysis is caused by the reticuloendothelial system, which is located predominantly in the spleen.
Reaction to incompatible transfusions and autoimmune hemolytic anemia are the two most prevalent causes of in vivo hemolysis. It is rare to see in vivo hemolysis, with just 3% of all hemolyzed samples undergoing this process. Yet in vivo hemolysis is of considerable therapeutic significance since it reveals an underlying disease condition in the patient. After different types of samples (eg, citrate, serum, and heparinated tube) have been hemolyzed over a longer period of time, or after repeated blood sampling has been done, even after particular care has been taken to prevent hemolysis.
The most obvious and specific laboratory indications of in vivo hemolysis are decreased amounts of haptoglobin in serum and free hemoglobin in urine. In the circulation, haptoglobin prevents hemoglobin from oxidatively damaging the body. In the plasma once it is liberated from the erythrocytes, hemoglobin is found in complexes with haptoglobin, which are then removed from circulation by macrophages. Haptoglobin can be undetectable in serum in severe cases of in vivo hemolysis (below the detection range), but its concentration in in vitro hemolysis remains stable.
Spectrophotometric interference
Spectrophotometric interference of hemolysis is caused by hemoglobin’s capacity to absorb light at wavelengths of 415nm, 540nm, and 570nm as a result of hemoglobin’s optical interference, measured parameters might be erroneously raised or lowered. Both the analyte and the technique have a significant impact on the interference’s direction and intensity.
Release of the Cell Components into the Sample:
Cellular concentrations of certain components are many times greater in blood than they are in the extracellular environment (ie, plasma or serum). illustrates some of the most significant discrepancies between intracellular and extracellular concentrations in red blood cells. In perspective of LDH, hemolysis has the most impact. Mild hemolysis can raise LDH activity by over 20%, whereas moderate hemolysis can increase it by over 60% and severe hemolysis can increase it by over 350%.
There is a substantial variation in potassium content between serum and plasma because intracellular components may escape from platelets during coagulation. Potassium concentrations in serum and plasma differ by an average of 0.36 0.18 mmol/L, and this difference is positively correlated with platelet count. In order to accurately assess potassium, plasma is the preferred sample type.
Sample Dilution:
The quantities of several analytes in plasma are significantly greater than those in blood cells. These include albumin, bilirubin, glucose, salt, and others. As a result of hemolysis, the concentrations of those parameters will be reduced in hemolyzed samples. Dilution bias only becomes clinically meaningful when hemolysis is severe.
Chemical Interference:
As a result of direct or indirect competition for molecules in reagents, inhibition of indicator reactions, or modification of analyte by complex formation, proteolysis, or precipitation, various blood cell components may impact the analyte measurement technique. For instance, Adenylate kinase is an enzyme that catalyzes the reversible conversion of ATP and AMP to two ADP molecules and maintains the adenine nucleotide cell content. When released from cells during hemolysis, it may compete for ADP with creatine kinase in a phosphoryl phosphatase assay. In another instances, through the suppression of the production of diazonium salt, free hemoglobin liberated from erythrocytes has pseudo-peroxidase activity that interferes with bilirubin concentration assays.
Hemolysis may cause a wide range of interference in immunochemistry assays. Interference is caused by modifying the reaction analytes (antigens and antibodies) by the proteolytic action of cathepsin E in mature erythrocytes. For example, current troponin assays have variable susceptibility to hemolysis interference. cTnT, insulin, cortisol, testosterone, and vitamin B12 concentrations have been found to be negatively affected by hemolysis.It has also been found to produce false-positive elevations in PSA and cTnI, which are dependent on the concentration of hemolysis. Analyte and method-specific biases, on the other hand, can affect the degree and direction of bias.
Lipemia
As the name suggests, lipemia is a visible turbidity in a sample that can be seen with the naked eye. The big lipoprotein particles in the sample produce turbidity in the sample by scattering light. Postprandial triglyceride elevation, parenteral lipid infusions, and certain lipoprotein diseases are the most frequent causes of a rise in lipoprotein levels in the bloodstream. Some lipoproteins contribute more to turbidity than others.
Spectrophotometric Interference:
As a result of light absorption and scattering, lipemia creates interference. When a light beam passes through the lipemic sample, its intensity is reduced as a result of light absorption by the sample. In the 300–700 nm wavelength region, lipoprotein particles have the capacity to absorb light. When wavelengths are reduced, sample absorbance increases and reaches a maximum in the UV range. Lipemia affects several enzymatic techniques that detect the final product at 340 nm (NAD[P] or NADP[H]).
Interference Caused by the Volume Depletion Effect:
Only a small fraction of lipids (10% of the total plasma volume) are present in fasting plasma of healthy persons. Most of the plasma is made up of water. Increasing the quantity of lipoprotein particles increases the amount of lipids in the bloodstream. The lipids displace particles that are not lipid soluble to the water portion of the plasma. The result of lipemia is that all techniques that assess analyte concentration in the total plasma volume will show a misleading reduction in that analyte’s concentration.
Interference Caused by Partitioning of the Sample:
When lipemic samples are centrifuged, lipoproteins are not evenly dispersed due to the lipid gradient. When it comes to lipid-soluble analytes, such as medicines and certain hormones that dissolve in fat, they are more concentrated in the top layer of the lipid-rich plasma or serum than water-soluble analytes. Particularly in automated chemical analyzers, where the sample probe has a set route length, this is critical. Analytes with unequal distribution across the lipid and water portions of the sample may provide different tests depending on where the sample probe is inserted.
Interference Caused by Physicochemical Mechanisms:
In electrophoresis and chromatography, an overabundance of lipoproteins in the blood can cause aberrant peaks. Elevated amounts of triglycerides and lipoprotein particles can affect the electrophoretic pattern and morphology, as well as erroneously increase the relative percentage of prealbumin, albumin, and α1- and α2-globulin regions. Moreover, lipemia may interfere with several immunochemistry experiments by obscuring the binding sites on antigens and antibodies and therefore physically interfering with antigen-antibody interaction.
Removing lipids from the sample:
Hemolysis, Icterus, and Lipemia/Turbidity Indices as Indicators of Interference in Clinical Laboratory Analysis (CLSI C56-A) recommends ultracentrifugation for removing excess lipids from samples. In order to clear lipemic sera, ultracentrifuges separate the lipids, notably chylomicrons, from the aqueous component (lower layer) of the sample using a centrifugation force of approximately 200,000 g.
Ultracentrifugation
Ultracentrifugation is a gold standard; however, it is not commonly available. For this reason, high-speed centrifugation utilizing a microcentrifuge with a centrifugation speed of up to 20,000 g is the preferred approach. In lipemic samples, the concentration of lipids determines the efficacy of high-speed centrifugation (HSC). Ultracentrifugation, on the other hand, is preferable than high-speed centrifugation for samples that are very lipemic. A 7-fold drop in triglyceride concentration can be achieved with the ultracentrifuge (from 59.2 to 8.1 mmol/L; or 5239 to 717 mg/dL), whereas a 3.4-fold reduction can be achieved with the high-speed centrifuge.
Lipid-clearing agents
Many laboratories employ lipid-clearing agents because of their low cost, simplicity, and ease of use. In addition to extracting lipids from a lipemic sample (cyclodextrin), these agents (polyethylene glycol, dextran, hexane, and others) may also reduce the quantity of protein in the lipemic sample. As a result, it is crucial for labs to check the performance of such reagents before using them on a regular basis, as they may not be suitable for a wide range of analytes due to their low recovery.
Icterus
Plasma (or serum) contains bilirubin in amounts up to 20 micrograms per milliliter (mg/L). When bilirubin concentration surpasses 34 mol/L, a change in the color of the serum (or plasma) can be detected. When bilirubin concentrations above 100 micromol/L, icterus is diagnosed. Patients in critical care units, gastrointestinal facilities, and pediatric clinics often have icteric plasma. Bilirubin interferes with numerous chemistry tests, including enzymes (ALT, alkaline phosphatase, creatine kinase, lipase), electrolytes, metabolites (urea, creatinine, glucose), lipids (cholesterol, triglycerides), proteins (albumin, total proteins, IgG), hormones (estradiol, beta-HCG, free T3), and even some drugs (gentamicin, phenobarbital, theophylline, tobramycin).
Icteric interference is difficult to eliminate or minimize in labs. The use of bilirubin oxidase as well as blanking techniques has been advocated by experts. Testing the necessary analytes with a different technique or on a different equipment where icterus does not produce clinically significant interference are possible solutions.
Spectrophotometric Interference of Bilirubin:
By absorption of light between 400 and 540 nanometers, the bilirubin produces interfering measurements in spectrophotometry.
Chemical Interference of Bilirubin:
Bilirubin generates a negative bias in assays that use H2O2 as an intermediate reaction (eg, cholesterol, glucose, uric acid, triglycerides).
Hemolytic, Icteric and Lipemic Samples Detection
Serum indices may be detected by visual inspection and by the use of automated detection systems. Hemolysis becomes visible at the concentration of 0.3 to 0.5 g/L of free hemoglobin, and the intensity of the red color of the serum or plasma further increases with the increase in free serum hemoglobin. Lipemia causes sample turbidity, which approximately corresponds to the percentage of serum triglycerides. Increased concentrations of serum bilirubin lead to yellow to orange-red coloration.
Visual evaluation of the degree of hemolysis, lipemia, and icterus is unreliable and can lead to mistakes. Hemolysis is the most frequent preanalytical mistake and the leading cause of sample rejection. Hemolysis may induce clinically meaningful bias through spectrophotometric and chemical interference, sample dilution, and the release of cell components into the sample. Lipemia produces interference through spectrophotometric interference (light absorption and light scattering), the volume depletion effect, partitioning of the sample, and physicochemical processes (eg, disturbance of the electrophoretic pattern).
Because of their poor recovery, lipid removal reagents may not be suitable for a wide range of analytes. Bilirubin comes in a variety of forms that interfere in variable degrees with different laboratory techniques, and even the identical forms of bilirubin behave differently with the same assays on different machines.
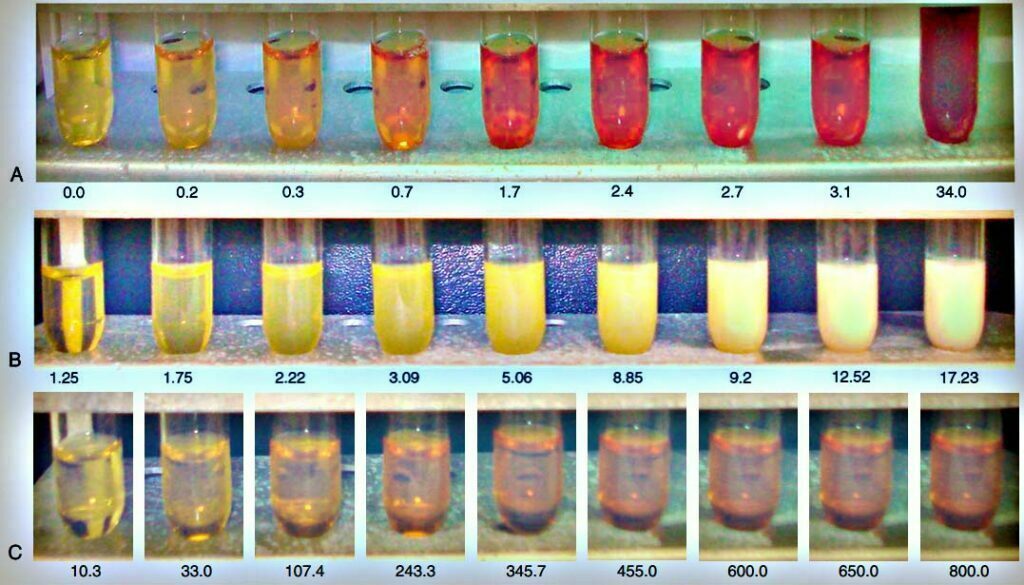
A, Hemolysis: the intensity of the red color of the serum and corresponding concentrations of free serum hemoglobin (in g/L).
B, Lipemia: the degree of turbidity and corresponding concentrations (in mmol/L) of tryglicerides.
C, Icterus: the intensity of the yellow color of the serum and corresponding concentrations of bilirubin (in µmol/L).
Drug induced interferences
Drug interferences in laboratory tests can be classified as biological or chemical, depending on the mode of action. Drugs and their metabolites can have biological effects when they act in vivo. Drugs can affect the results of a wide range of tests in a variety of ways.
- Induction of microsomal enzymes in the liver (phenytoin raises levels of gamma-glutamyl transferase through this mechanism)
- By inhibiting 5α-reductase, finasteride and dutasteride reduce prostate-specific antigen levels.
- Substances displaced from the protein-binding location (tizoxanide alters free warfarin fraction by its displacement from the protein-binding site; this effect can be monitored by alterations in coagulation parameters)
Due to structural similarities, the parent drug or its metabolite may interfer with immunochemical or photometric techniques. Chemical or immunochemical reactions can be interfered with when the substance, or its metabolites, accelerate or inhibit certain processes. Some medications can alter the sample density (viscosity) and cause difficulties with analytical equipment by interfering with sample integrity (eg, iodinebased contrast media).
Interferences in Immunoassays
Immunoassays are sensitive to a variety of preanalytical interferences, and not all assays are equally susceptible to all interfering factors. Hence, lab workers should be well-versed in their particular tests and tools, along with potential sources of interference. Assays involving immunochemistry are described below in terms of key preanalytical concerns.
Potentially Interfering Tube Additives in Immunoassays:
By interfering with antigen-antibody binding and response rate, heparin interferes with a wide range of immunoassay methods. It has been shown that heparin plasma causes a substantial negative bias in cardiac troponin detection when used with several previous generations troponin tests from many major manufacturers. Observed bias did not associate with cardiac troponin concentrations. Due to its negative charge and its binding to positively charged troponin, heparin interferes with troponin’s signaling.
Heparin and troponin binding causes a conformational shift in troponin, which alters the antibody-antigen interaction. To counteract this interference, the fourth-generation troponin T test was modified by adding an inhibitor of cationic heparin to the mix of the assay, although there are still instances where serum and plasma results cannot be compared with each other. A consistent sample type for troponin testing for a specific patient is therefore necessary. EDTA’s primary role is chelation. Higher quantities of EDTA in a sample increase its chelating activity.
Formation of Fibrin Clots:
New tube types with clot activators (thrombin-based clotting agent) have shortened serum clotting time (on average 2.5 minutes) without affecting sample quality and stability for most chemical analytes. As a result of delayed and latent clotting, insoluble fibrin, fibrin strands, and microclots may impair instrument performance and produce interferences. While some analyzers have the capacity to identify clots and indicate them as needing to be repeated, clots can interfere with assay measurements and result in inaccurate findings and needless delays if this function is not accessible. Cardiac troponin tests have been plagued by mistakes owing to latent clotting or inadequate fibrin removal during centrifugation, and laboratories have tried a variety of techniques to reduce the possibility of reporting erroneous findings due to fibrin clots.
Interference due to Separator Gels
Separator gels are used to ensure fast and persistent separation of serum/plasma from clots of blood and cells. Due to the gel’s specific gravity (1.03–1.06), its capacity to undergo a transient change in viscosity during centrifugation, and its tendency to lodge between the packed cells and the top serum/plasma layer, the sample can be separated. For this reason, tubes with separator gels should not be used for hydrophobic medicines and hormones such as the following:
- Drugs: phenytoin, phenobarbitol, carbamazepine, tricyclic antidepressants, quinidine, lidocaine
- Hormones: testosterone, estradiol, cortisol, free thyroxine, total triiodothyronine
Due to variations in gel composition among various manufacturers, it is conceivable that one manufacturer’s gel tube can be used for a certain analyte, while another manufacturer’s gel tube cannot. Moreover, if inappropriate storage conditions (time and temperature) are followed, the gel may breakdown and release tiny particles or globules into the supernatant. These particles can interfere with instrument performance by interfering with the sample probe, covering the inner surface of reaction cuvettes, and interfering with immunoassays. As a result, it’s vital to closely adhere to the storage and handling instructions supplied by the tube makers.
Paraprotein interferences
A variety of analytical equipment have shown paraprotein interference, which appears to be depending on the analytical technique and concentration. Several processes, including precipitation, volume displacement, and change in sample viscosity, might cause paraprotein interference in chemical tests. When paraprotein reacts with the solubilizing agent in the reagent used to detect total bilirubin levels, it might precipitate.
Paraproteins can bind to any component of the reaction mixture, including the analyte. The effect of such interference is determined by the component to which the paraprotein is attached. The binding of an IgM paraprotein to latex particles resulted in elevated CRP and antistreptolysin O (ASO) levels. Unlike turbidity, this type of interference does not affect the sample. This sort of interference cannot be identified by looking at the reaction curve on the instrument since the kinetics of the unaffected sample are extremely similar to that of the sample with an interfering paraprotein.
The volume displacement effect of paraproteins affects chemical tests in the same way as lipemia does. Changes in serum electrolytes, particularly serum sodium, are most noticeable with indirect ion-selective technology (ISE). When sodium is measured by indirect ISE, a high quantity of paraproteins causes misleading hyponatremia.
Paraproteins can interfere simply by changing the viscosity of the sample. Viscosity is significantly greater in samples with extremely high paraprotein concentrations or in chilled samples where a gel has formed (as in cryoglobulinemia). The volume of the sample pipetted into the reaction mixture is affected by sample viscosity.
Reference:
- Tietz Textbook of Clinical Chemistry