
Table of Contents
Introduction
Gonorrhea is one of the most prevalent sexually transmitted infections (STIs) worldwide, caused by the bacterium Neisseria gonorrhoeae. The name “gonorrhea” originates from the Greek words meaning “flow of seed,” reflecting the misconception in ancient times that its symptoms were due to semen discharge. Historically, gonorrhea and syphilis were often confused, with gonorrhea initially thought to be an early stage of syphilis in the 16th century. The infection has also been commonly referred to as “the clap,” a term believed to have derived from the French word clapoir, meaning “brothel.”
Transmission and Symptoms
Gonorrhea spreads through direct contact with infected bodily fluids via vaginal, anal, or oral sex. The bacteria thrive in warm, moist areas such as the urethra, cervix, uterus, fallopian tubes, and even the throat and rectum.
Symptoms in Women:
- Vaginal discharge (white, yellow, or green)
- Painful urination
- Increased urinary frequency
- Abdominal or pelvic pain
- Painful intercourse
- Fever (in severe cases)
- Sore throat (if contracted through oral sex)
Symptoms in Men:
- Painful urination
- Penile discharge (clear, white, yellow, or green)
- Red or swollen urethra
- Testicular pain or swelling
- Sore throat (if contracted through oral sex)
Many individuals, particularly women, may experience asymptomatic infections, increasing the risk of complications such as pelvic inflammatory disease (PID) and infertility if left untreated
Pathophysiology
Growth and metabolism
N. gonorrhoeae is highly sensitive to environmental changes, including temperature fluctuations, dehydration, and oxygen levels. The bacteria survive by acquiring essential nutrients such as iron from human proteins like transferrin and hemoglobin. Their ability to adapt to different oxygen levels within the urogenital tract allows them to colonize various environments.
Resistance and Genetic Adaption
Most N. gonorrhoeae strains carry plasmids encoding resistance to antibiotics, particularly penicillin and tetracyclines. These include the African, Asian, and Rio/Toronto plasmids, which contribute to high-level antimicrobial resistance.
Colonization determinants
To establish infection, N. gonorrhoeae utilizes various virulence factors:
- Metal transport mechanisms: Help in nutrient uptake
- Type IV pili: Essential for adhesion to host cells
- Opa proteins: Aid in immune system evasion
- PorB porin: Helps in nutrient acquisition
- Efflux pumps: Provide resistance to antimicrobial agents
Complications and Host Damage
Unlike some bacterial infections, gonorrhea does not produce exotoxins but releases toxic components like peptidoglycan fragments and outer membrane vesicles. This contributes to inflammation, tissue damage, and scarring, particularly in the fallopian tubes, leading to PID, infertility, and ectopic pregnancy. In rare cases, disseminated gonococcal infections (DGIs) can cause:
- Fever
- Dermatitis
- Septic arthritis
- Endocarditis
- Meningitis
Clinical Presentation and Laboratory Diagnosis
The incubation time for urogenital gonorrhea varies from ~2 days to 8 days. The clinical signs of gonorrhea are heterogeneous and vary substantially in men and women. Laboratory diagnosis of gonorrhea is established by direct identification of the organism in urogenital, anorectal, pharyngeal, or conjunctival swab specimens or first-catch urine.
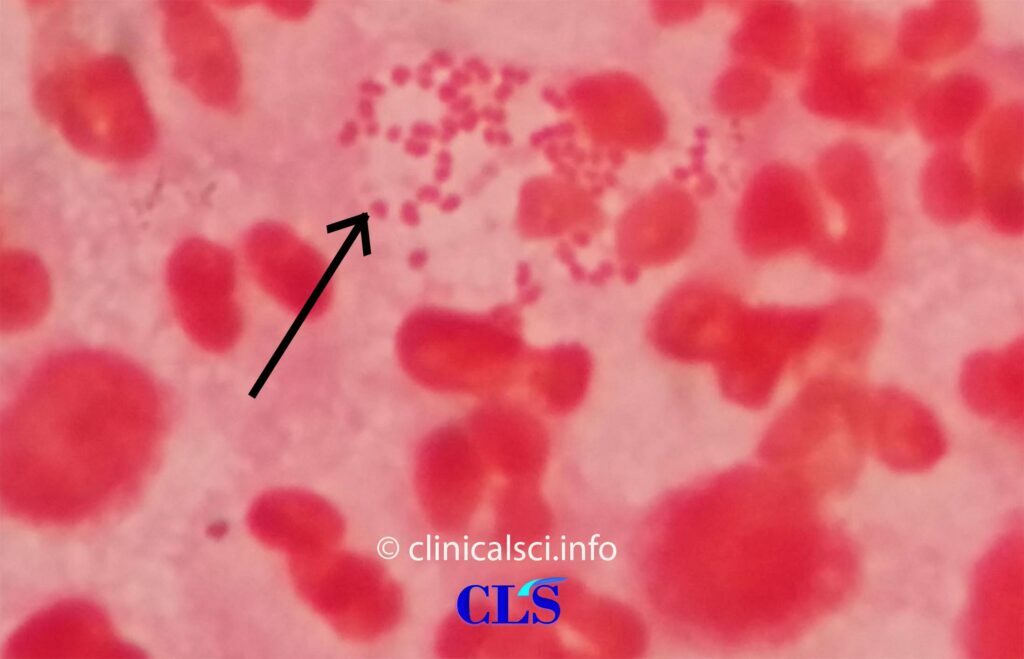
Microscopy
Methylene blue staining and Gram’s staining are adopted for direct microscopy. The slide is covered with a 1 % aqueous methylene blue. The preparation is washed with water and dried after a brief exposure (15 s). When bacteria are stained with methylene blue, they all become blue. It should only be used in conjunction with normal clinical signs to diagnose simple male urethritis.
Gram’s staining is essential in female’s gonorrhea and all other indications of disease. Commercially available staining packages are also available. Gram stain is ineffective for diagnosing Neisseria gonorrhoeae from pharyngeal or rectal specimens (since other Neisseria species with similar appearance are common in the oral and nasopharyngeal cavities).
Culture
Antimicrobial resistance in Neisseria gonorrhoeae is a serious issue all over the globe, and reliable findings are required for an effective treatment. Bacterial culture is very particular and sensitive. Under ideal circumstances, sensitivity in urogenital specimens may reach 85–95 %, and specificity can approach 100 % when species identification is conducted.
Gonococci are fastidious pathogens. They do not tolerate dehydration and should be inoculated into culture media shortly after swab collection (nutritious selective culture medium and non-selective culture medium). Culture plates must be incubated at 35–37°C, high humidity (70–80%), pH 6.75–7.5, and in a 4–6% CO2-enriched environment. After 18–24 (~48) h, tiny, glossy gray colonies form, allowing for colony growth fluctuations. Following cultivation, the identity of Neisseria gonorrhoeae is determined by combining different detection techniques.
A microscopic Gram’s staining preparation and positive cytochrome oxidase reaction are used to achieve a preliminary identification. Biochemical studies, immunological testing, spectrometric tests, or molecular tests are used to confirm the identification and discriminate between other Neisseria species, such as Neisseria meningitidis and apathogenic Neisseria spp., particularly in extragenital areas.
Antimicrobial Susceptibility Testing
The WHO-recommended gold standard technique for antimicrobial susceptibility testing in Neisseria gonorrhoeae is agar dilution. An antibiotic agent is integrated into a nutrient medium in a defined series of strengths. The corresponding inhibition zone is read off as the antibiotic concentration increases. The MIC value in μg/ml (mg/l) is the lowest concentration that inhibits growth. However, this procedure is sophisticated and best suited to a large variety of tests. As a result, the standardized and quality-assured MIC gradient stripe test technique (Etest), which correlates with the agar dilution method, is presently the preferred method.
Nucleic Acid Amplification Technologies (NAATs)
NAATs are currently a major diagnostic test since specimen collection is noninvasive (urine or self-collected swabs, particularly vaginal swabs); live organisms are not required for detection. This facilitates less restrictive transportation and storage procedures.
NAATs are also the most efficient tests for detecting extragenital Neisseria gonorrhoeae infection and are so recommended for laboratory detection of rectal or pharyngeal infection. Further have a glance at FDA approved NAAT tests.
Rapid/POCT tests
Despite the fact that NAATs are considered the standard tests for detecting Neisseria gonorrhoeae, their application in low- and middle-income countries is severely constrained due to their relatively expensive prices. Given the availability of a microscope, microscopy may be regarded a Neisseria gonorrhoeae RDT that can be conducted at the point of care. Microscopic examination, on the other hand, necessitates expert investigators and lacks sensitivity in asymptomatic infections as well as anorectal and pharyngeal specimens. However, some lateral flow immunoassays are also available.
Treatment and Antibiotic Resistance
Gonorrhea treatment has become increasingly challenging due to antimicrobial resistance. Current CDC guidelines recommend dual therapy with:
- Ceftriaxone (500 mg intramuscularly, single dose)
- Azithromycin (1g orally, single dose) or Doxycycline (100 mg twice daily for 7 days) (if chlamydia co-infection is suspected)
In cases of multidrug-resistant N. gonorrhoeae, alternative antibiotics such as gentamicin or cefixime may be considered.
Prevention and Public Health Strategies
Prevention Measures:
- Safe sex practices: Use of condoms.
- Regular STI screenings: Especially for sexually active individuals with multiple partners
- Partner notification and treatment: To prevent reinfection
- Vaccination research: While no vaccine exists yet, ongoing research aims to develop one
Conclusion
Gonorrhea remains a significant public health concern due to its high prevalence and increasing antibiotic resistance. Early detection through NAATs, culture testing, and antimicrobial susceptibility assessments are crucial for effective treatment. Prevention strategies, including safe sex practices and regular screenings, play a vital role in controlling the spread of this infection. Ongoing research into novel antibiotics and potential vaccines provides hope for improved management in the future.l antibiotics and potential vaccines provides hope for improved management in the future.
References:
- Bailey Scott’s Diagnostic Microbiology 14th Edition
- Textbook of Diagnostic Microbiology by Connie R Mahon 6th Edition
- Meyer, T., & Buder, S. (2020). The Laboratory Diagnosis of Neisseria gonorrhoeae: Current Testing and Future Demands. Pathogens (Basel, Switzerland), 9(2), 91. https://doi.org/10.3390/pathogens9020091
- Unemo, M., Seifert, H.S., Hook, E.W. et al. Gonorrhoea. Nat Rev Dis Primers 5, 79 (2019). https://doi.org/10.1038/s41572-019-0128-6