
Introduction
Syphilis remains a globally relevant sexually transmitted infection (STI), despite modern prevention and treatment strategies. Early detection and timely treatment are essential to prevent long-term complications such as neurosyphilis, cardiovascular syphilis, or congenital transmission. The VDRL (Venereal Disease Research Laboratory) and RPR (Rapid Plasma Reagin) tests are cornerstone tools in syphilis screening.
Though these tests are widely used, many clinicians and laboratory personnel misunderstand their limitations, interpretation pitfalls, and when confirmatory testing is necessary. A deep, meticulously referenced, and up-to-date guide can help bridge that gap.
VDRL and RPR: Basic Concepts
What are non-treponemal tests?
- VDRL and RPR are non-treponemal (or non-specific) serologic tests. They detect reagin antibodies — antibodies directed against lipoidal antigens (i.e., cardiolipin‑lecithin complexes) released from damaged host cells or the treponemes themselves.
- They do not directly detect Treponema pallidum (the syphilis-causing spirochete). Because of this, any positive result must be confirmed by a treponemal (specific) test, such as FTA-ABS (Fluorescent Treponemal Antibody Absorption), TPHA (Treponema pallidum hemagglutination), or newer immunoassays.
Why two tests (VDRL vs RPR)?
- The VDRL test is a classical flocculation assay requiring a microscope.
- The RPR test is a modified version that uses carbon particles (i.e. charcoal) to permit macroscopic reading, eliminating the need for a microscope, and simplifying workflow.
- In many clinical laboratories, RPR is preferred for screening because it is faster, more convenient, and easier to automate.
- However, in certain scenarios — e.g. cerebrospinal fluid (CSF) evaluation for neurosyphilis — VDRL remains the preferred non-treponemal test.
Laboratory Procedure for VDRL and RPR Tests
1. Sample Collection
- Serum sample:
- Collect 5 mL of venous blood in a plain, red-top tube (no anticoagulant).
- Allow the blood to clot at room temperature for 30–60 minutes.
- Centrifuge at 1500–2000 g for 10 minutes to separate serum.
- Carefully collect the serum, avoiding hemolysis.
- CSF sample (for VDRL):
- Collect 1–2 mL of cerebrospinal fluid (CSF) by lumbar puncture, ideally before antibiotic therapy.
- CSF should be processed within 2 hours or stored at 4°C if delayed.
- No heat inactivation is required for CSF samples.
2. Serum Inactivation (VDRL Test Only)
- Heat inactivation is recommended to destroy complement proteins and prevent non-specific reactions.
- Incubate the serum sample at 56°C for 30 minutes in a water bath.
- Allow serum to cool to room temperature before proceeding with the test.
- Note: RPR does not typically require serum inactivation due to its different antigen system.
3. Sample Volume for Testing
- Use 0.05 mL (50 µL) of serum or CSF per test reaction for both VDRL and RPR.
4. Reagents
- VDRL antigen: Cardiolipin-cholesterol-lecithin suspension, provided in a standardized vial.
- RPR antigen: Cardiolipin suspension coated with carbon particles for visible clumping.
5. Test Procedure
a. VDRL Test (Serum and CSF)
- For serum:
- Place 0.05 mL of heat-inactivated serum on a clean glass slide or test card.
- For CSF:
- Place 0.05 mL of fresh CSF directly (no heat inactivation) on the slide.
- Add 0.05 mL of VDRL antigen suspension to the sample.
- Mix thoroughly by rotating the slide gently for 4 minutes at room temperature (20–25°C).
- Examine under a microscope at 10x or 20x magnification for flocculation (clumping).
- A positive test shows fine, granular, particulate clumps swirling on rotation.
b. RPR Test (Serum Only)
- Place 0.05 mL of non-inactivated serum on a white plastic or glass card.
- Add 0.05 mL of RPR antigen containing carbon particles.
- Mix immediately with a plastic stirrer for 8 minutes at room temperature.
- Observe macroscopically for black clumping due to carbon particle aggregation.
- Positive reaction appears as visible aggregates clumping together.
6. Controls
- Use positive and negative control sera for each test batch to validate results.
- Controls must give expected results: positive control shows flocculation; negative control remains smooth.
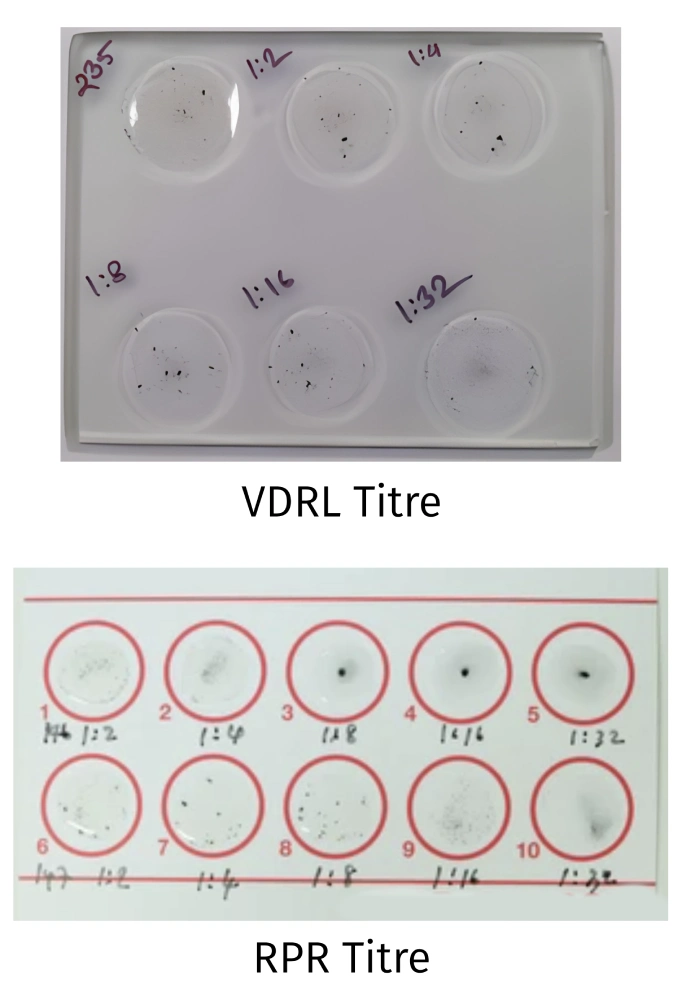
7. Titration (Quantitative Testing)
- If screening test is reactive, perform serial two-fold dilutions (1:2, 1:4, 1:8, etc.) with saline or buffer.
- Test each dilution with equal volume of antigen (0.05 mL).
- The highest dilution showing flocculation corresponds to the antibody titer.
8. Precautions and Notes
- Avoid excessive shaking to prevent false positives.
- Use fresh serum samples and perform tests within recommended time frames.
- CSF testing is only performed with VDRL, not RPR.
- Temperature and timing are critical for reproducibility.
- Report any reactive CSF VDRL as diagnostic for neurosyphilis but correlate clinically.
Summary Table: Laboratory Procedure Overview for VDRL and RPR Tests
| Test | Sample Type | Serum Inactivation | Sample Volume (mL) | Mixing Time | Observation Method |
| VDRL (Serum) | Serum (heat-inactivated) | Yes (56°C for 30 min) | 0.05 | 4 minutes | Microscopic (10x or 20x) |
| VDRL (CSF) | CSF (fresh) | No | 0.05 | 4 minutes | Microscopic (10x or 20x) |
| RPR | Serum (non-inactivated) | No | 0.05 | 8 minutes | Macroscopic (naked eye) |
Interpretation of Results
Qualitative (screening) results
- Non-reactive / Negative: No visible flocculation or clumping.
- Reactive / Positive: Visible flocculation or clumping
- Weakly reactive / equivocal: Borderline changes; may require repeat or confirmatory testing
- Prozone suspicion: If a sample tests nonreactive despite high clinical suspicion or other positive tests, serial dilutions may reveal reactivity.
Quantitative titers
- The titer is the highest dilution factor (e.g., 1:4, 1:16, 1:64) at which reactivity is still observed.
- Rising titers over serial testing (e.g. 1:8 → 1:32) suggest active or untreated infection
- Declining titers (e.g. 1:32 → 1:4) after therapy indicate treatment response
- However, titers do not fall to zero in all patients; some patients remain serofast (i.e., persistent low-level positivity).
Sensitivity and specificity by stage
The performance of non-treponemal tests depends strongly on the stage of syphilis:
| Stage | Approx. Sensitivity (VDRL / RPR) | Comments |
| Primary syphilis | ~ 62–78% (some reports as low as 50%) | Antibody levels may be too low early on |
| Secondary syphilis | ~ 97–100% | Most reliable stage for detection |
| Early latent (<1 year) | ~ 82–100% | May vary depending on definition |
| Late latent / unknown duration | ~ 63–66% | Sensitivity declines |
| Tertiary syphilis | ~ 47–64% | Lower sensitivity due to lower antibody levels |
| Neurosyphilis (CSF) | VDRL: 49–87.5% | RPR (CSF): 51.5–82% |
Thus, in early and late stages, false negatives are more likely. It underscores why combining serologic, clinical, and sometimes CSF studies is essential.
Clinical contexts:
- Treponemal confirmation: A reactive non-treponemal test alone does not confirm syphilis; a treponemal-specific test is mandatory.
- History and prior treatment: Previously treated patients may have persistent low-level reactivity (serofast).
- Serial measurements: Single titers are less meaningful than trends over time.
- Prozone effect: Always consider in cases of strong suspicion but negative result.
- Cross-reactions / biologic false positives: Must be excluded.
Clinical Significance & Use Cases
Screening and diagnosis
- VDRL and RPR are first-line screening tools for syphilis in many settings (antenatal screening, STI clinics, blood banks).
- For example, a large study of approximately 9,347 pregnant individuals reported RPR sensitivity of about 90.86% and specificity of around 99.57%, comparable to VDRL..
- In mass screening, the low cost and simplicity of these tests make them extremely useful.
- RPR may be more favorable in resource-limited, high-volume settings, due to ease of use and minimal equipment needs.
Antenatal Screening
- RPR is widely used for routine syphilis screening during antenatal check-ups to prevent congenital syphilis.
- Early detection enables timely treatment, reducing fetal and neonatal complications.
- Due to its rapid, low-cost nature and ease of use, RPR is ideal for high-volume prenatal settings, especially in resource-limited areas.
- Guidelines recommend testing at the first prenatal visit, with repeat tests in high-risk cases.
Monitoring treatment response
- Declining titer (usually a fourfold or greater drop, e.g. 1:32 → 1:8) over 6–12 months indicates effective therapy.
- Persistent titers without rise suggest serofast state, not necessarily treatment failure.
- If titers increase (e.g. 1:8 → 1:32), this suggests reinfection or treatment failure.
Neurosyphilis evaluation
- When neurosyphilis is suspected (neuro symptoms, ocular involvement, HIV co-infection, etc.), CSF-VDRL remains a gold standard non-treponemal test, despite moderate sensitivity.
- CSF-RPR has lower sensitivity and is not considered superior to CSF-VDRL.
- Be cautious: a nonreactive CSF-VDRL does not exclude neurosyphilis; diagnosis relies on clinical correlation and possibly other CSF parameters (e.g. pleocytosis, elevated protein, or treponemal antibodies).
Public health surveillance and epidemiology
- In epidemiological studies and syphilis surveillance, non-treponemal tests allow quantitative trends across populations (titers rise or decline).
- Their cost-effectiveness makes large-scale screening feasible.
Limitations, Pitfalls, and False Results
No diagnostic test is perfect. Below is a detailed breakdown of common challenges with VDRL and RPR assays.
Biologic false positives
Non-treponemal tests can be reactive in a variety of non-syphilis conditions. Table adapted from literature:
| Condition | Mechanism or Notes |
| Infectious diseases | HIV, viral hepatitis, malaria, mononucleosis, leprosy, bacterial endocarditis, pneumonia, tuberculosis, chancroid |
| Autoimmune / connective tissue disease | SLE, rheumatoid arthritis, antiphospholipid syndrome |
| Pregnancy | Physiological antibodies may cause mild reactivity |
| Aging / chronic disease | Older age, malignancies, chronic liver disease |
| Recent immunization or vaccination | Transient reactivity may occur |
| Injection drug use, trauma, recent blood transfusion | Tissue damage may liberate cardiolipin-like antigens |
This is often called a biologic false positive (BFP) response. Because of this, any reactive non-treponemal result should be followed by a confirmatory treponemal test.
False negatives
Causes include:
- Prozone (antibody excess): When antibody concentration is extremely high, it interferes with flocculation formation in undiluted serum. Serial dilution helps.
- Low antibody titers: Especially in very early infection (window period) or late latent disease.
- Technical errors: Poor antigen prep, improper mixing, using plasma for VDRL, cold centrifugation.
- Post-zone effect or antigen excess (rare but possible): misbalance of antigen‑antibody ratio.
- Treponemal sequestration: In tertiary disease, antibodies may be sequestered in tissues rather than freely circulating.
- In neurosyphilis: CSF-VDRL or CSF-RPR can be negative despite disease.
Serofast state
Some treated patients continue to have low-level reactive non-treponemal titers over long periods (months to years) without evidence of active infection. This serofast status is not uncommon.
Inter-test non-equivalence
- Although RPR is often slightly more sensitive, VDRL and RPR titers are not interchangeable. In one study, only ~29% of sera had concordant titers between RPR and VDRL. PMC
- Laboratories should stick to one test platform when monitoring a patient over time.
Laboratory variability / quality control
- Reagent lot differences, human error, sample handling, and reading subjectivity can affect results.
- Rigor in standard operating procedures, calibration, and external quality assessment is vital.
Clinical false positives (due to cross-reactions)
- In regions endemic for nonvenereal treponematoses (e.g. yaws, pinta), non-treponemal tests may be positive due to cross-reactivity. But titers are usually low (e.g. <1:8).
- This underscores the importance of epidemiologic context.
Comparative Summary: VDRL vs RPR
Below is a side-by-side summary of advantages, disadvantages, and ideal use contexts:
| Feature | VDRL | RPR |
| Observation | Microscopic (flocculation) | Macroscopic (carbon particles) |
| Need for heat inactivation | Yes (serum) | No (antigen modified) |
| Antigen stability | Fresh daily prep | More stable, ready-to-use reagents |
| Equipment requirement | Microscope, rotator | Card rotator (no microscope) |
| Throughput / ease | Slower, more labor-intensive | Faster, suitable for automation |
| Use in CSF (neurosyphilis) | Preferred non-treponemal test | Less reliable in CSF |
| Sensitivity / specificity | Good, but lower in many settings | Slightly higher sensitivity in many studies |
| Titer comparability | Good for tracking | Good for tracking — but do not mix with VDRL in same patient series |
Thus, RPR is often preferred for routine screening, while VDRL maintains value in neurosyphilis workup and certain settings.
Best Practices & Recommendations
To maximize accuracy and reduce misleading results, labs and clinicians should follow these guidelines:
- Use confirmatory treponemal testing for all reactive non-treponemal results
- Avoid mixing assay types within a patient’s serial follow-up
- Check for prozone effect if negative but strong clinical suspicion (repeat at dilutions)
- Use serial titers, not a single result, to judge trends
- Consider the clinical context (history, symptoms, risk factors)
- Evaluate CSF in suspected neurosyphilis regardless of negative serum result
- Participate in external quality assurance
- Document reagents, lot numbers, technician identity, and reading conditions
- Be cautious in populations prone to false positives (autoimmune disease, pregnancy, endemic areas)
- Report lower limit of detection and alert clinicians on low titers
Conclusion
The VDRL and RPR tests remain foundational tools in syphilis screening and monitoring, combining affordability with practical value. Yet, their use requires nuanced understanding of laboratory technique, result interpretation, and limitations. To summarize:
- These are non-treponemal, screening assays detecting reagin antibodies, not Treponema pallidum itself
- RPR is often preferred in clinical practice for its ease, speed, and macroscopic reading
- VDRL, especially in CSF, retains importance for neurosyphilis evaluation
- Interpretation should always include quantitative titers, clinical context, and confirmation with treponemal assays
- Pitfalls include false positives (autoimmune, infections, aging, pregnancy), false negatives (prozone, low titer), and serofast persistence
- Laboratories should adopt best practices, QC procedures, and reagent validation
For clinicians and lab managers, the practical takeaway is: use non-treponemal tests wisely as a screening and monitoring tool, always confirm positives, monitor trends, and interpret results in context. With careful technique and understanding, VDRL and RPR remain indispensable in syphilis control.
FAQ
Q1: How soon after syphilis exposure can VDRL or RPR tests detect antibodies?
Typically, non-treponemal tests become positive about 2–4 weeks after infection (sometimes longer). In very early (primary) infection, false negatives are common due to low titers.
Q2: If my VDRL/RPR test is positive, do I need more tests?
Yes, a treponemal-specific test (e.g. FTA-ABS, TPHA, TPPA, immunoassay) is required to confirm the diagnosis and rule out false positives.
Q3: Can a previously treated patient show a positive non-treponemal test later?
Yes, many patients enter a serofast state where low-level reactivity persists over time without evidence of active infection.
Q4: Why might a sample test negative when clinical suspicion is high?
Possible causes include the prozone effect, low antibody titers (early or late disease), or technical issues. Serial dilution and repeat testing help.
Q5: Which test is better: VDRL or RPR?
Neither is universally superior. RPR is more convenient, faster, and easier to use in routine screening. VDRL remains useful in CSF testing and special contexts. The key is consistency and proper interpretation.
References
- Centers for Disease Control and Prevention. (2024). CDC Laboratory Recommendations for Syphilis Testing. MMWR.
- Hook, E. W., III, & Peeling, R. W. (2021). “Syphilis Laboratory Guidelines: Performance Characteristics of Nontreponemal Antibody Tests.” Clinical Infectious Diseases, 71(Supplement_1), S21–S29.
- Holroyd, K. J., et al. (2022). Serological tests for syphilis. PMC article.
- Other peer-reviewed and authoritative sources as cited within text