
Table of Contents
Introduction
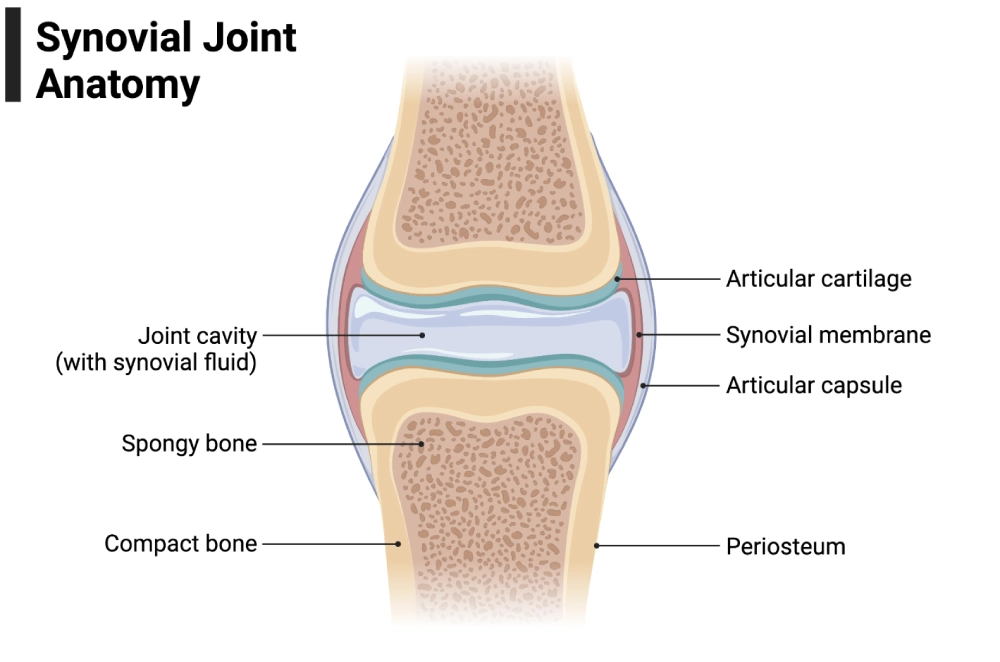
Synovial fluid is a clear, viscoelastic liquid within synovial (diarthrodial) joints, crucial for lubrication and joint health. Arthrocentesis, the aspiration of synovial fluid, serves as a “liquid biopsy” that aids diagnosis and treatment of joint diseases by relieving pressure and providing diagnostic clues for infections, crystal arthropathies, inflammatory, and degenerative conditions. Rapid and accurate synovial fluid analysis can distinguish between urgent septic arthritis requiring surgery and inflammatory arthritis manageable with medical therapy. (NCBI)
Common conditions evaluated with synovial fluid analysis include:
- Septic arthritis (including periprosthetic joint infection, PJI)
- Crystal arthropathies (gout due to monosodium urate [MSU]; calcium pyrophosphate deposition disease [CPPD])
- Inflammatory arthritis (e.g., rheumatoid arthritis, psoriatic arthritis, lupus arthritis)
- Noninflammatory effusions (e.g., osteoarthritis, traumatic effusions)
- Hemarthrosis (e.g., trauma, coagulopathy)
Synovial Fluid: Composition and Function
Synovial fluid is an ultrafiltrate of plasma enriched with hyaluronic acid and lubricin, which confer viscosity and lubricating properties. Normal joint fluid volume is approximately 1 mL in large joints. Under healthy conditions, it contains <200 white blood cells (WBCs)/µL, predominantly mononuclear cells, with no red blood cells (RBCs) or crystals. Its glucose and protein levels closely mirror plasma, with total protein <3 g/dL.
Normal Constituents of Synovial Fluid
- Cells: Very low WBC burden (<200 cells/µL), predominantly mononuclear cells (lymphocytes, monocytes, macrophages) with <25% neutrophils. RBCs and crystals are normally absent. Rare cytologic findings include neutrophages/Reiter cells (macrophages containing neutrophils) in reactive arthritis; LE cells may appear in SLE; eosinophils can be seen in select settings (e.g., after arthrography, parasitic infection, Lyme disease).
- Macromolecules: Hyaluronic acid (viscosity), lubricin/PRG4 (surface boundary lubrication), albumin/globulins, and surface-active phospholipids.
- Chemistry: Composition resembles plasma minus larger proteins; total protein <3 g/dL in healthy fluid. Glucose approximates serum glucose.
Indications for Synovial Fluid Analysis
Clinical Scenarios Prompting Joint Aspiration
Perform arthrocentesis whenever there is acute monoarthritis, a new or unexplained effusion, suspected septic arthritis, suspected crystal disease, or prosthetic joint complications. Arthrocentesis can both diagnose and alleviate symptoms by decompressing a tense joint. (NCBI)
Common Indications
- Hot, swollen joint with or without fever (rule out sepsis)
- Acute pain and swelling with suspected gout/CPPD
- Flare of rheumatoid arthritis or other inflammatory arthritides
- Prosthetic joint pain/loosening (evaluate for PJI)
- Hemarthrosis after trauma or in coagulopathy
- Chronic effusion of uncertain cause (consider TB, crystal disease, OA)
Specimen Collection and Handling
Arthrocentesis Technique
- Perform aseptic skin preparation and use sterile gloves and equipment.
- Use plastic syringes and disposable needles to avoid contamination with crystals.
- Site selection depends on joint involved; ultrasound guidance can aid aspiration.
- Aspirate maximum safe volume; allocate samples appropriately.
- For suspected infection, inoculate part of the specimen into blood culture bottles at bedside for improved organism recovery.
Sample Division and Tube Allocation
Ideally divide the specimen immediately:
- Sterile tube (no additive) for Gram stain and culture
- EDTA or heparin tube for cell count, differential, and microscopy (including crystals)
- Plain tube for chemistry (glucose, protein, LDH, lactate, uric acid, immunology tests)
Process samples quickly (within 1–2 hours), refrigerate if delay is unavoidable, and consider hyaluronidase treatment to reduce viscosity for cell counting.
Transport and Storage Guidelines
- Process rapidly ideally within 1–2 hours for cell counts and crystal detection to reduce cellular degeneration and loss of birefringence.
- Refrigerate (2–8 °C) if delays are unavoidable. Avoid freezing unless validated for a specific assay.
- Viscosity management for counts: If fluid is highly viscous and resists mixing or pipetting, treat an aliquot with 0.5% hyaluronidase in phosphate buffer for several hours to reduce viscosity; document that treatment was applied.
Laboratory Analysis of Synovial Fluid
Physical Examination
- Color & Transparency: Healthy fluid is straw‑colored and clear. Noninflammatory effusions are typically clear; as cells, proteins, or crystals increase, turbidity rises. A simple “newspaper test” reading print through a test tube, roughly gauges clarity.
- Viscosity: At the bedside, normal synovial fluid forms a 4–6 cm string as it drops from the needle. Breaking before ~3 cm suggests reduced viscosity from hyaluronate degradation in inflammation.
- Blood: A traumatic tap often shows decreasing blood in sequential tubes or streaks in the syringe; a true hemarthrosis is uniformly bloody throughout and tends not to clot. Xanthochromia in supernatant suggests older bleeding.
- Clotting: While normal synovial fluid does not clot, infectious and crystal‑induced effusions frequently form fibrin clots, which may impede counting unless an anticoagulant is used.
Interpretation of Physical Findings
- Cloudy/opalescent fluid indicates increased cells or crystals; opaque/purulent fluid raises concern for septic arthritis. However, appearance alone cannot diagnose or exclude infection—microscopy and culture are mandatory. (Merck Manuals)
Chemical Analysis
Routine chemistry is supportive and does not replace microscopy and culture:
- Glucose: Normally mirrors serum. A markedly low synovial glucose (compared with concurrently drawn serum) supports bacterial infection or, less commonly, active RA; interpret with the WBC and differential.
- Protein: Low in healthy (≈ one‑third of plasma; typically, <3 g/dL). In inflammatory and infectious conditions, protein level elevates.
- Lactate & LDH: Often elevated in septic arthritis and can support the diagnosis when combined with cellular findings; cutoffs vary by laboratory and are not standalone rules.
- Uric acid: May be checked in select contexts but has limited diagnostic value compared with crystal microscopy.
Clinical Interpretation of Chemical Results
- Very low glucose and high lactate favor septic arthritis, especially with high WBC and neutrophil predominance; however, no single chemistry result can rule in or out infection. (Merck Manuals)
Microscopic Examination
Cytologic Examination
- Total WBC count nd differential are essential for classifying joint effusions. A neutrophil predominance exceeding 75% is highly suggestive of septic arthritis but can also be observed in crystal-induced arthritis (NCBI). Therefore, a comprehensive evaluation, including crystal analysis, is crucial for accurate diagnosis.
- Neutrophil fraction: A neutrophil fraction of >75–90% or highers increases the likelihood of septic arthritis, but high neutrophil counts also occur in crystal flares. Do not exclude infection just because crystals are present. (SpringerOpen)
- Gram stain: Gram stain provides rapid but insensitive for native joint septic arthritis. Across studies, sensitivity is often ~25–40% with high specificity, a negative Gram stain does not rule out infection. Culture remains essential. (PMC)
- Cytology for malignancy: Malignant cells are rarely seen; correlation with clinical and imaging findings is required.
Note of WBC Counting: Automated counters and the use of Turk’s fluid are not recommended for WBC counting in synovial fluid, as they may cause clot formation and inaccurate results. Instead, validated manual counting methods consistent with CLSI H56 guidelines should be employed for reliable cell enumeration
Crystal Identification and Clinical Correlation
Why it matters: Crystal analysis is a unique and high‑yield feature of synovial fluid workups. If volume or resources are limited, crystal examination (with compensated polarized light) and microbiology should be prioritized.
Workflow & optics
- Prepare a fresh wet mount on a clean slide and coverglass; minimize contaminants (starch/glove powder). Seal the coverglass (e.g., clear nail polish) to prevent drying if prolonged observation is needed.
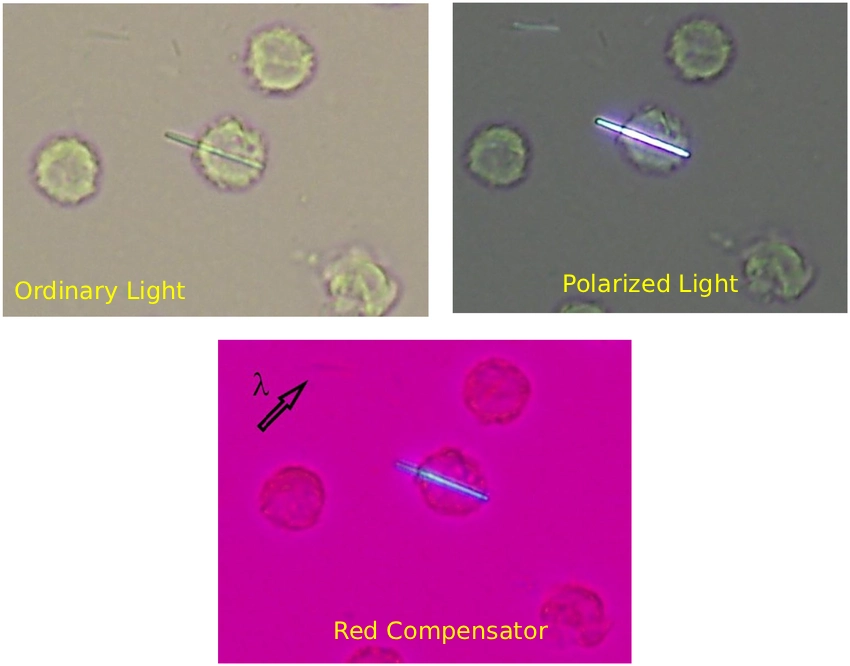
- Examine first with brightfield or phase‑contrast; then use polarized light with a first‑order red (full‑wave) compensator to determine birefringence sign.
- Report “crystals present/absent” and type; avoid the ambiguous phrasing “negative crystal exam.”
Crystal types
- Monosodium urate (MSU)
- Morphology: Long needle‑shaped or rods (1–30 µm).
- Birefringence: Strongly birefringent; negative birefringence—yellow when parallel to the slow axis of the compensator and blue when perpendicular.
- Clinical note: Finding MSU crystals in a symptomatic joint is the gold standard for gout diagnosis and overrides serum urate fluctuations. (ard.bmj.com)
- Calcium pyrophosphate (CPPD)
- Morphology: Rhomboid, rectangular, short rods; may be small and chunky (1–20 µm).
- Birefringence: Weak, positive birefringence—blue when parallel, yellow when perpendicular to the slow axis.
- Basic calcium phosphate (BCP) including hydroxyapatite
- Visibility: Particles are submicroscopic and not visible with routine polarized light. Screening with alizarin red S can detect calcium‑containing crystals but does not distinguish BCP from CPPD; specialized techniques are needed if BCP disease (e.g., Milwaukee shoulder) is suspected. PMC
- Artifacts and look‑alikes:
- Glove powder (starch) shows Maltese crosses; steroid crystals (iatrogenic) can resemble both MSU and CPPD; polyester fibers may appear after joint replacement; collagen, fibrin strands, and cartilage fragments can confuse interpretation.
Avoid:
- Delays reduce crystal yield, examine immediately.
- Document hyaluronidase treatment if used; it can improve smear quality but should be applied to a separate aliquot.
- Crystals and infection can coexist; don’t stop once crystals are found if clinical suspicion for infection remains. SpringerOpen
Synovial Fluid Classification Systems
The following table summarizes widely used patterns. Ranges overlap; always integrate with clinical context.
| Parameter | Normal | Noninflammatory (OA/trauma) | Inflammatory (RA, gout, CPPD) | Infectious (Septic) | Crystal‑Induced (Gout/CPPD) | Hemorrhagic |
| Appearance | Clear, straw | Clear–yellow | Cloudy–opalescent | Opaque, purulent; may be green/milky | Yellow/turbid | Uniformly bloody |
| Viscosity | High | High | Low | Very low | Low–variable | Variable |
| WBC (cells/µL) | <200 | <2,000 | 2,000–50,000 (± higher) | >50,000 (often >100,000) | 500–200,000 | Variable; RBC present |
| % Neutrophils | <25% | <25% | >50% | >75–90% | Up to 90% | Variable |
| Glucose vs serum | Similar | Similar | Normal or mildly ↓ | Markedly ↓ | Usually normal | Similar |
| Protein | <3 g/dL | Near normal | ↑ | ↑↑ | ↑ (variable) | Variable |
| Clot formation | None | None | Sometimes | Common | Common | Variable |
Selected values and descriptors are adapted from standard clinical sources and the provided text; exact cutoffs vary by laboratory. (Merck Manuals)
Common Synovial Fluid Findings by Disease
- Gout (MSU crystal arthritis)
- Profile: Inflammatory; WBC often 10,000–70,000/µL with neutrophil predominance.
- Definitive test: MSU crystals with negative birefringence on compensated polarized light. Serum urate can be normal during flares; the crystal exam is decisive.
- CPPD (pseudogout)
- Profile: Overlaps gout; inflammatory WBC range with neutrophil predominance.
- Definitive test: CPP crystals (rhomboid/rods), weak positive birefringence. Coexists with OA and can be associated with hypothyroidism, hyperparathyroidism, and hemochromatosis
- Septic arthritis (native joint)
- Profile: Classically >50,000 WBC/µL (often >100,000) and >90% neutrophils, with low glucose and elevated lactate; however, counts below 50,000 occur and do not exclude infection. Gram stain is specific when positive but has low sensitivity; culture is essential. Inoculating blood culture bottles increases recovery.
- Rheumatoid arthritis
- Profile: Inflammatory (WBC typically 2,000–50,000/µL); reduced viscosity. Occasional LE cells and ragocytes may be seen; immunoglobulins in synovial fluid can approach serum levels.
- Osteoarthritis
- Profile: Noninflammatory; WBC <2,000/µL, high viscosity, clear. It may contain cartilage fragments or collagen fibrils on phase‑contrast microscopy.
- Tuberculous arthritis
- Profile: Subacute; moderate WBC often with lymphocyte predominance. AFB smear of synovial fluid has low yield; culture and synovial biopsy are more sensitive. NAATs/PCR (e.g., Xpert MTB/RIF) can provide rapid results and detect rifampin resistance, but performance varies and approval may be specimen‑type dependent. (PMC)
- Hemarthrosis
- Profile: Uniformly bloody fluid, often nonclotting; consider trauma, tumor, anticoagulation, or bleeding diathesis.
Ancillary Tests and Emerging Biomarkers
Modern markers support (not replace) core microscopy and culture:
- Alpha‑defensin: Synovial alpha‑defensin shows high diagnostic accuracy for periprosthetic joint infection (PJI) in meta‑analyses, with ELISA generally outperforming lateral‑flow assays. False positives may occur (e.g., metallosis), and cost and availability vary. (PubMed)
- Calprotectin: A neutrophil-derived protein measurable by lateral‑flow or laboratory assays. Meta‑analyses suggest strong “rule‑out” performance for chronic PJI, making it a practical adjunct. (PMC)
- Interleukin‑6 (IL‑6): Elevated in synovial fluid during PJI and shows high diagnostic accuracy in systematic reviews; platform thresholds vary, and IL‑6 works best combined with synovial WBC and %PMN. (PMC)
- Leukocyte esterase (LE) strips: Fast and inexpensive; results are operator‑dependent and should be interpreted with cell counts and culture.
- Lactate (including D‑lactate): Elevated in infection; promising as a supportive marker but with heterogeneous cutoffs that require local validation.
Use biomarkers within validated diagnostic frameworks (e.g., contemporary MSIS/ICM criteria for PJI) and in multidisciplinary discussion. (PubMed)
Routine Examination Checklist
- Gross appearance: color, clarity (“newspaper test”), viscosity (string test), volume, clots.
- Cellular analysis: total WBC and differential (treat a separate aliquot with hyaluronidase if viscosity impairs handling).
- Crystal analysis: brightfield/phase‑contrast → polarized light with compensator; report present/absent and type.
- Microbiology: Gram stain and culture; blood culture bottles for suspected infection (plus sterile tube).
- Chemistry/immunology: glucose (with paired serum), protein, LDH, lactate; consider RF, ANA, complement in specific scenarios.
Common Limitations and How to Avoid Them
- Treating Gram stain as a gatekeeper. A negative Gram stain does not exclude septic arthritis; its sensitivity is limited. Proceed with culture and integrate clinical/lab findings.
- Overreliance on a single WBC cutoff. The often‑quoted 50,000/µL threshold has limited sensitivity; septic joints can present with lower counts, and crystal flares can exceed it. Use the full context (WBC, %PMN, glucose, lactate, risk factors).
- Delayed crystal examination. Time degrades birefringence; examine immediately and refrigerate if delayed.
- Improper tube allocation. Divide into sterile, EDTA/heparin, and plain tubes; avoid gel separators. Adhere to CLSI H56 and your lab’s SOPs.
- Ignoring dual pathology. Crystals and infection can coexist; maintain suspicion if systemic signs persist or cultures are pending.
Conclusion
Synovial fluid analysis is one of the most impactful and cost‑effective diagnostics in musculoskeletal medicine. Success begins at the bedside with meticulous aseptic collection, thoughtful sample division, and rapid processing and continues at the bench with disciplined microscopy, judicious chemistry, and appropriate microbiology. Crystal identification under compensated polarized light remains uniquely powerful, while recognition of the limitations of Gram stain and WBC cutoffs prevents misdiagnosis. In prosthetic joints, biomarkers such as alpha‑defensin, calprotectin, and IL‑6 add speed and nuance when interpreted within validated criteria.
Frequently Asked Questions
What does cloudy synovial fluid indicate?
Cloudiness usually reflects increased cells, crystals, or suspended debris/lipids. In inflammatory and septic arthritis, hyaluronidase activity degrades hyaluronate, lowering viscosity and increasing turbidity. Opaque, purulent fluid raises concern for infection and warrants immediate Gram stain and culture.
How is gout diagnosed in synovial fluid?
The gold standard is finding needle‑shaped, negatively birefringent MSU crystals under compensated polarized light in a symptomatic joint. ACR/EULAR classification criteria support diagnosis when crystal analysis is unavailable, but documented crystals trump all.
What is the normal white blood cell count in synovial fluid?
Normal synovial fluid has <200 WBC/µL with <25% neutrophils. Noninflammatory effusions are generally <2,000/µL. Always interpret results alongside the differential and clinical context.
Can synovial fluid tests detect cancer?
Occasionally. Cytology may show malignant cells when tumors involve the synovium or metastasize to the joint, but this is uncommon. Suspicious cases warrant imaging and tissue diagnosis.
Why compare synovial glucose with serum glucose?
Because synovial glucose approximates serum in health. A substantially lower synovial glucose (from a sample drawn concurrently with serum) supports infection, especially when paired with a high WBC and neutrophil predominance.
References
- Brunzel, N. A. (2018). Fundamentals of Urine and Body Fluid Analysis (4th ed.). Philadelphia, PA: Elsevier/Saunders. (Primary details incorporated throughout this article.)
- Clinical and Laboratory Standards Institute (CLSI). (2019–2024). H56: Body Fluid Analysis for Cellular Composition. Wayne, PA: CLSI.
- Merck Manual Professional. (2024). Acute Infectious Arthritis. Retrieved 2025.
- Neogi, T., Jansen, T. L., Dalbeth, N., et al. (2015). 2015 gout classification criteria: An ACR/EULAR collaborative initiative. Annals of the Rheumatic Diseases, 74(10), 1789–1798.
- Vale, J. S., Pitta, M., et al. (2023). Synovial fluid biomarkers for the diagnosis of periprosthetic joint infection: Systematic review and meta‑analysis. The Journal of Arthroplasty.
- Cohen, D., et al. (2020). Synovial fluid culture: Agar plates vs. blood culture bottles for septic arthritis. Journal of Infection and Public Health.