
Table of Contents
Introduction
Hargraves et al., identified the LE cell phenomena in bone marrow in 1948. Lupus erythromatosus is an autoimmune disease in which autoantibodies attack cell nuclei components. In lupus erythromatosus, antibodies such as LE factor, antinuclear antibodies (ANA), anti double stranded DNA (anti ds DNA), anti single stranded DNA, anti nucleoprotein, and anti nuclear glycoprotein are detected.
Lupus is a connective tissue disease, characterized by skin rash (mostly butterfly like), arthralgia, fever, renal, cardiac and vascular lesions, anemia, leucopenia and often thrombocytopenia. It involves chronic inflammation that can affect many parts of the body, including: Heart, lungs, skin, joints, blood-forming organs, kidneys, nervous system. Lupus can occur at any age however it is most common in women of child bearing age and children.

Types of Lupus Erythromatosus
Lupus erythromatosus can present as a systemic or mainly cutaneous illness. The following are examples of lupus erythromatosus types:
- Systemic lupus erythematosus (Most common and severe form)
- Drug-induced lupus erythematosus
- Neonatal lupus erythematosus
- Acute cutaneous lupus erythematosus
- Subacute cutaneous lupus erythematosus
- Discoid lupus erythematosus ( chronic cutaneous)
Formation of LE cells
The LE factor (ANF), an immunoglobulin of the IgG, IgM, or IgA class, is released during the process of LE cell formation. The ANF causes the release of an enzyme called DNAse, which depolymerizes the nuclear chromatin of polymorphonuclear leucocytes. This depolymerized DNA creates the LE body, a solid, homogeneous mass with chemotactic potential for polymorphs. As a result, other non-traumatic neutrophils phagocytose the LE body, causing LE cells to develop.
LE cells are often neutrophils, however they can also be monocytes or eosinophils. When a neutrophil engulfs the nucleus of another polymorph, these cells create a spherical, opaque, darkly coloured, uniform purple-brown mass. The engulfing cell’s lobes appear to be wrapped around the engulfed material. In some cases, a collection of polymorphs may surround a modified nuclear material to form a “rosette” shape.
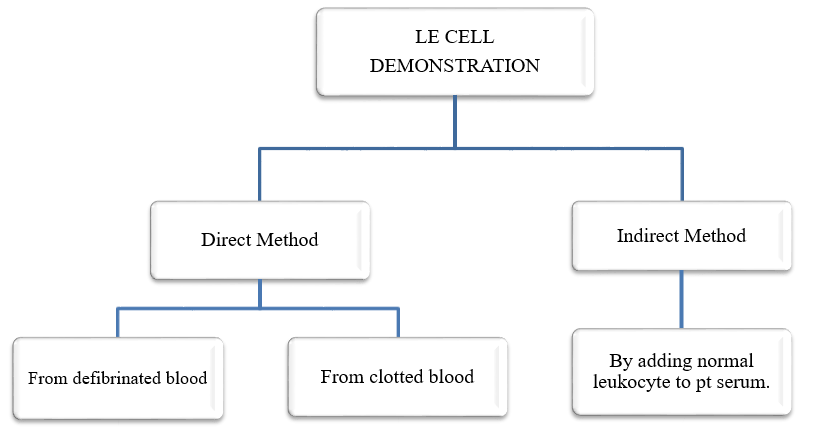
Demonstration of LE cells
3 / 3
Several approaches may be used to display LE cells, however it appears that some amount of stress on white blood cells is required for an efficient preparation. White blood cells do not respond to the LE factor while they are alive and healthy. To produce LE cells, white blood cells must be exposed to conditions which lead them to become stressed. When they are stressed, the LE factor might cause the creation of the characteristic LE cells.
3 / 3
Rotating the whole blood sample with glass beads before centrifugation can assist to prepare LE cells. This procedure aids in the concentration of white blood cells and the creation of some amount of damage, both of which are required to properly exhibit LE cells. Because healthy white blood cells are unable to respond to the LE factor, which is essential to generate LE cells, the damage caused by the rotation with glass beads is required.
Method Using Patient’s Blood
The Rotary Method of Zinkham and Conley
- 1 mL of heparinized patient blood is transferred to a 75 x 12mm glass tube.
- The tube is sealed with a securely fitting rubber bung after four glass beads are inserted.
- For 30 minutes, the preparation is spun at 33 rpm at room temperature before being put in a 37°C oven for 10-15 minutes.
- Transfer the contents of the tube to a Wintrobe tube and centrifuge for 10 minutes at 200g.
- Buffy coat smears are made, air-dried, fixed with methanol, then stained with Romanowsky stain as specified.
Examination of Films
- The L.E. cell is a neutrophillic leucocyte that is dilated by an intracytoplasmic homogeneous red purple body, i.e. the L.E body, and the phagocyte cell, which appears larger than normal.
- A negative report is issued after scanning the films for at least 10 minutes (counting at least 500 polymorphs). It is common to observe dead nuclei laying around; if they are abundant, they may raise suspicions, but they are not diagnostic.
Sometimes, instead of LE cells, you might see the “tart cells” which are usually monocytes that have ingested a lymphocyte’s nucleus. Tart cells have a distinct appearance than LE cells, and they can be observed in some patients under medications or as well as other medical disorders.
Interpretation
- A positive test result, as reported in 75% of SLE patients, is strongly suggestive of the disease, making it a helpful diagnostic tool.
- False positive findings, however, have been recorded in individuals with lupoid hepatitis, severe and very active rheumatoid arthritis, and those on medication treatment.