
Nipah virus (NiV) is a highly pathogenic zoonotic virus that poses a significant global health threat due to its high mortality rate, human-to-human transmission, and the lack of approved vaccines or antiviral therapies. Since its discovery in Malaysia and Singapore (1998-1999), NiV has caused recurrent outbreaks in South and Southeast Asia, particularly in Bangladesh and India, with a case fatality rate exceeding 50%. This virus is primarily transmitted through direct contact with infected animals, consumption of contaminated food, or human-to-human transmission.
NiV infection is known to cause severe acute febrile illness and progressive encephalitis. Respiratory complications are also common, with the virus displaying a pronounced tropism for endothelial cells and neurons, leading to vasculitis and microvascular injury. This complex pathogenesis not only influences clinical outcomes but also dictates the diagnostic approach in clinical practice.
The laboratory diagnosis of Nipah virus requires a multimodal approach, integrating molecular techniques such as real-time reverse transcription polymerase chain reaction (RT-PCR) with serological assays for antibody detection. Although advanced diagnostic platforms, such as high-sensitivity immunoassays and genomic sequencing, enhance detection and outbreak investigation, challenges such as biosafety containment and limited access to specialized laboratories remain critical factors in diagnosis, particularly in resource-limited settings.
Taxonomic Classification and General Characteristics
Nipah virus belongs to:
- Order: Mononegavirales
- Family: Paramyxoviridae
- Genus: Henipavirus
Henipaviruses are characterized by their broad host range, ability to infect endothelial and neuronal tissues, and capacity for zoonotic spillover. Unlike many paramyxoviruses that primarily cause self-limiting respiratory illness, Nipah virus causes systemic infection with high fatality, reflecting its unique structural and functional attributes.
Nipah virus is an enveloped virus, a feature that enhances environmental sensitivity but also facilitates efficient host cell entry via membrane fusion mechanisms. The presence of a lipid envelope, derived from the host cell membrane, has important implications for specimen handling, viral inactivation, and disinfection protocols in laboratory settings.
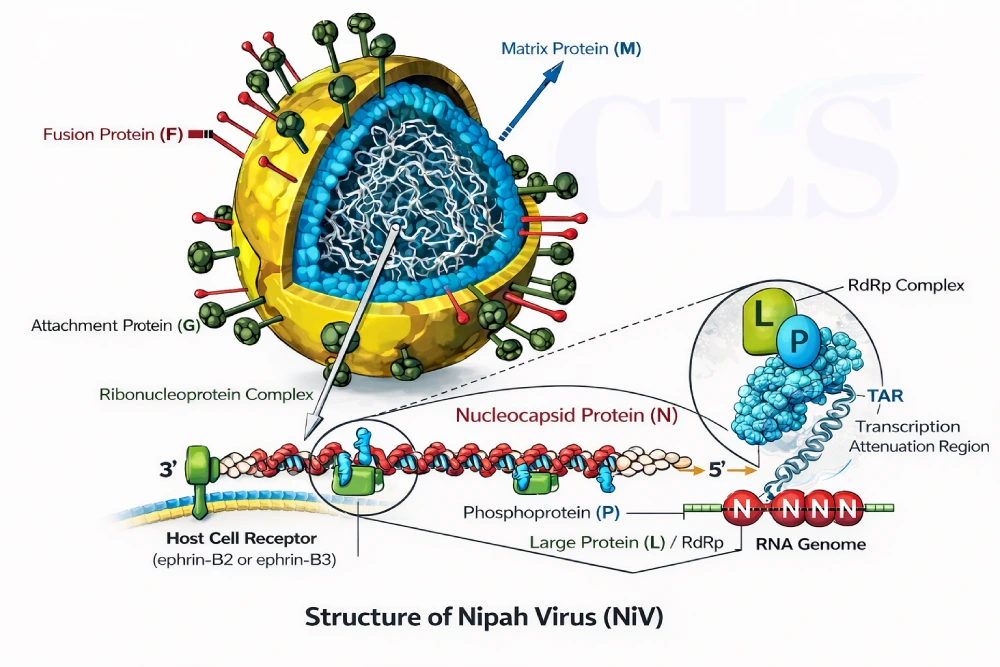
Structure of Nipah Virus
Nipah virus exhibits several structural features that distinguish it from other paramyxoviruses and contribute to its exceptional virulence.
Genome Organization and Molecular Composition
Nipah virus contains a non-segmented, negative-sense single-stranded RNA genome approximately 18.2 kilobases in length. The genome follows a conserved paramyxoviral gene order.
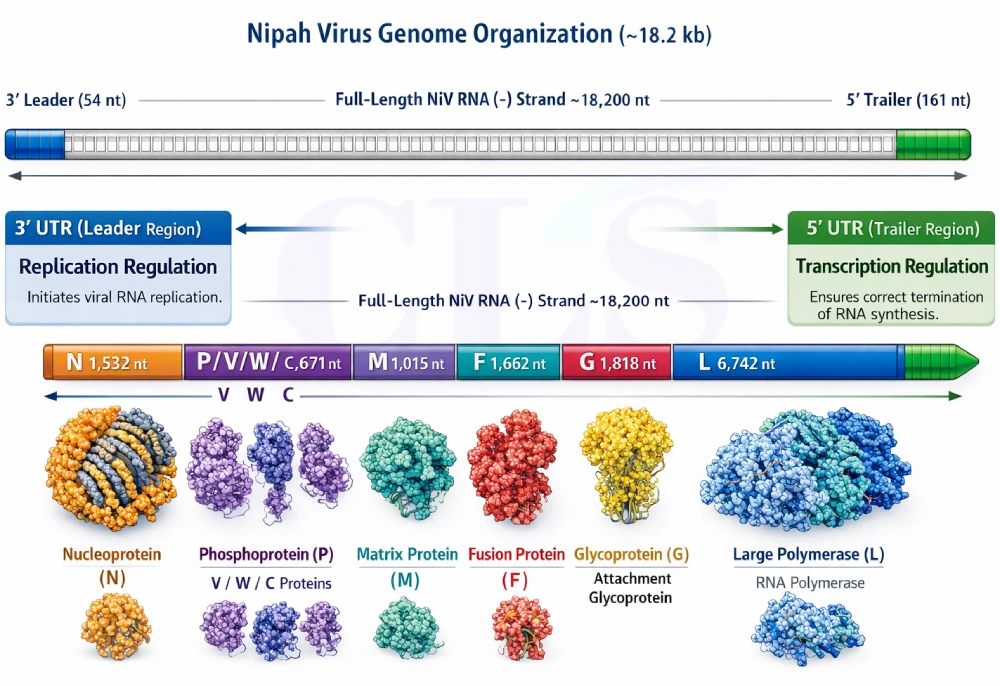
Each gene is flanked by transcription start and stop signals, resulting in sequential transcription by the viral polymerase complex. This transcriptional gradient leads to higher expression of genes located at the 3′ end of the genome, particularly the nucleocapsid protein gene.
- Genes with higher transcript abundance (such as N and P genes) are preferred targets for RT-PCR assays, as they improve analytical sensitivity.
Nucleocapsid Protein (N)
The nucleocapsid protein encapsulates the viral RNA genome, forming a helical ribonucleoprotein (RNP) complex. This complex protects viral RNA from degradation and serves as the template for transcription and replication.
Key characteristics include:
- High conservation across Nipah virus strains
- Strong RNA-binding capacity
- Abundant expression during infection
Phosphoprotein (P) and Accessory Proteins
The phosphoprotein functions as a cofactor for the viral RNA-dependent RNA polymerase. Through RNA editing, the P gene also encodes multiple non-structural proteins, including V, W, and C proteins, which play essential roles in immune evasion.
These proteins interfere with host antiviral defenses by suppressing interferon signaling pathways, thereby enhancing viral replication and persistence.
Matrix Protein (M)
The matrix protein lines the inner surface of the viral envelope and plays a critical role in virion assembly and budding. It acts as a bridge between the nucleocapsid and the envelope glycoproteins.
From a structural standpoint, the M protein ensures proper virion morphology and stability. While not commonly targeted in diagnostic assays, it is essential for understanding viral assembly and release.
Fusion Protein (F)
The fusion protein is synthesized as an inactive precursor (F0) and is cleaved by host cell proteases into two subunits, F1 and F2. This cleavage is essential for membrane fusion activity.
Once activated, the F protein mediates:
- Fusion of viral and host cell membranes
- Formation of multinucleated syncytia
- Efficient cell-to-cell viral spread
Attachment Glycoprotein (G)
The attachment glycoprotein is the primary determinant of host cell specificity. It binds with high affinity to ephrin-B2 and ephrin-B3 receptors, which are widely expressed on endothelial cells, neurons, and respiratory epithelial cells.
This receptor usage explains:
- Severe neurological involvement
- Widespread vascular damage
- Respiratory manifestations
Antigenic and diagnostic importance
- The G protein is the dominant antigenic target for neutralizing antibodies.
- It is widely used in serological assays, including ELISA and advanced luminescent immunoassays.
- Structural stability and conservation make it suitable for high-specificity diagnostic platforms.
Large Protein (L): RNA-Dependent RNA Polymerase
The L protein is the catalytic core of the viral polymerase complex. It is responsible for:
- Transcription of viral mRNA
- Replication of the viral genome
- RNA capping and methylation
Recent structural studies have revealed a highly organized polymerase complex, underscoring its essential role in viral replication and pathogenicity.
Virion Morphology and Envelope Characteristics
Nipah virus virions are pleomorphic, ranging from spherical to filamentous forms. The viral envelope contains host-derived lipids embedded with F and G glycoproteins.
Antigenic Structures of Nipah Virus
Nipah virus possesses a limited but highly functional antigenic repertoire, with surface and internal proteins eliciting distinct immune responses. Among these, the viral envelope glycoproteins, particularly the attachment glycoprotein (G), play a significant role in both the virus’s infectivity and its diagnostic utility.
Attachment Glycoprotein (G)
- The attachment glycoprotein (G) is the primary antigenic determinant of Nipah virus and is crucial for host cell binding, particularly to ephrin-B2 and ephrin-B3 receptors on endothelial cells, neurons, and respiratory epithelial cells.
- Key Antigenic Features:
- The G protein contains highly conserved conformational epitopes that serve as the primary targets for neutralizing antibodies.
- Laboratory diagnostic relevance: G protein is widely used in serological assays (e.g., ELISA) to detect antibodies during infection and in vaccine development.
Fusion Protein (F)
- The fusion protein (F) facilitates viral entry into host cells by mediating the fusion of the viral and host cell membranes.
- The F protein is cleaved into two subunits (F1 and F2) by host proteases, which are essential for the fusion process.
- Antigenic Characteristics:
- Contains both linear and conformational epitopes.
- Antibodies targeting the F protein exhibit neutralizing activity, though generally to a lesser extent than those targeting the G protein.
Nucleocapsid Protein (N)
- The nucleocapsid protein (N) encapsidates the viral RNA genome, forming a helical ribonucleoprotein (RNP) complex.
- Antigenic Role:
- The N protein is highly conserved and is abundant during infection, making it a key target for serological assays that detect IgM and IgG antibodies.
- It is useful for diagnosis in the acute and convalescent phases of infection.
Phosphoprotein (P) and Accessory Proteins
- The phosphoprotein (P) and associated accessory proteins (V, W, and C) play critical roles in viral replication and immune evasion, but they are less relevant as diagnostic antigens due to variable and inconsistent antibody responses.
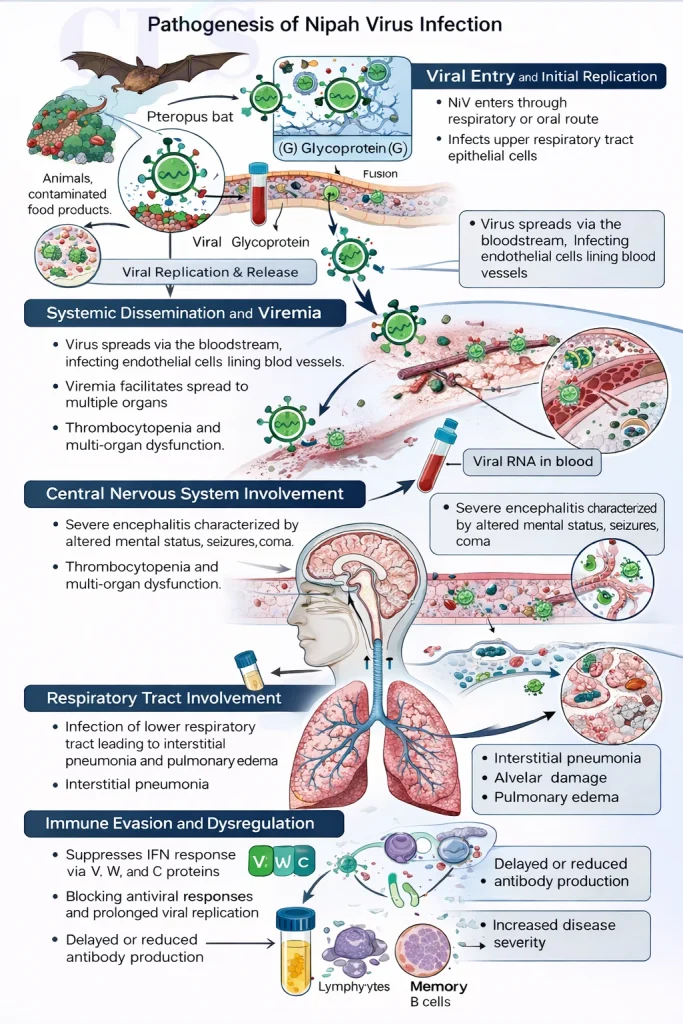
Pathogenesis of Nipah Virus Infection
The pathogenesis of Nipah virus infection involves multiple stages, including efficient viral entry, systemic dissemination, immune evasion, and tissue damage. The virus has a marked tropism for neurons and endothelial cells, which contributes to its high case fatality rate.
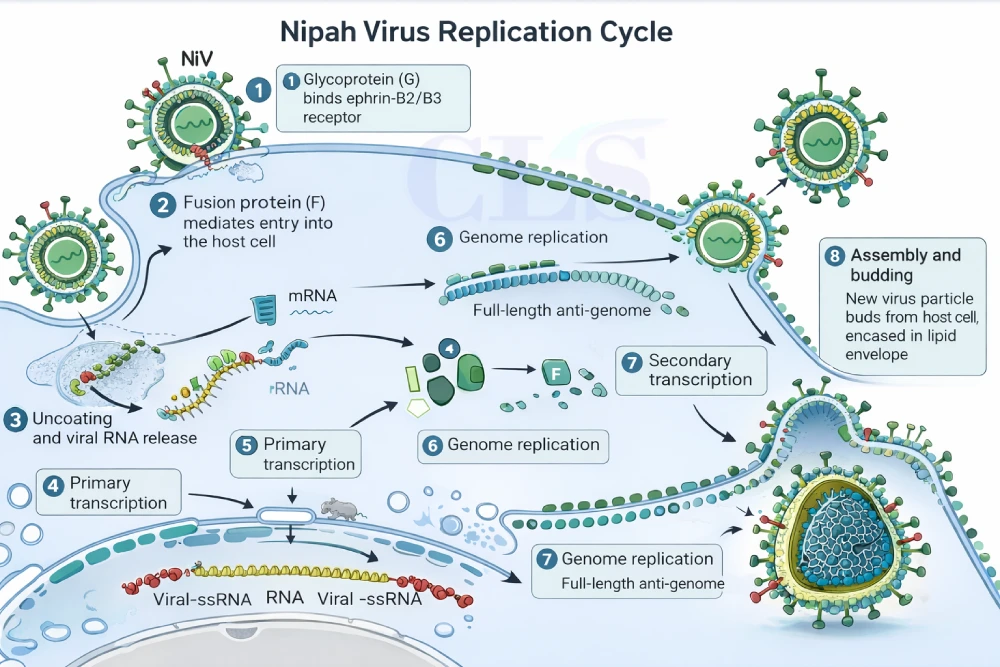
Viral Entry and Initial Replication
Nipah virus enters the human host primarily through the respiratory or oral route, following exposure to infected animals, contaminated food products, or respiratory secretions from infected individuals. Upon entry, the virus initially infects epithelial cells of the upper respiratory tract or oropharyngeal mucosa.
Attachment of the virus to host cells is mediated by the interaction between the viral G glycoprotein and the ephrin-B2 and ephrin-B3 receptors. These receptors are highly conserved and widely expressed in multiple tissues, facilitating rapid viral spread beyond the site of entry. Following attachment, the F glycoprotein mediates fusion of the viral envelope with the host cell membrane, allowing release of the nucleocapsid into the cytoplasm.
Laboratory relevance
- Early viral replication in respiratory tissues supports the use of throat or nasopharyngeal swabs for molecular detection during the initial phase of illness.
- High viral replication at entry sites contributes to the risk of human-to-human transmission, emphasizing early laboratory confirmation.
Systemic Dissemination and Viremia
After local replication, Nipah virus disseminates systemically via the bloodstream, leading to viremia. The virus exhibits a strong tropism for endothelial cells lining blood vessels, which serves as a critical step in disease progression.
Infected endothelial cells undergo degeneration and necrosis, resulting in widespread vasculitis, increased vascular permeability, and microvascular thrombosis. These vascular changes facilitate viral access to multiple organs, including the brain, lungs, spleen, and kidneys.
Clinical laboratory implications
- Detection of viral RNA in blood during the viremic phase supports the use of plasma or serum samples for RT-PCR.
- Endothelial damage contributes to laboratory abnormalities such as thrombocytopenia, elevated inflammatory markers, and evidence of multi-organ dysfunction.
Central Nervous System Involvement
One of the defining features of Nipah virus infection is severe involvement of the central nervous system. The virus gains access to the brain through both hematogenous spread and possibly via infected endothelial cells of the blood–brain barrier.
Within the CNS, Nipah virus infects neurons and glial cells, leading to:
- Neuronal necrosis
- Perivascular inflammation
- Microinfarctions
- Cerebral edema
These pathological changes manifest clinically as acute encephalitis, characterized by altered mental status, seizures, and coma. In some patients, neurological deterioration is rapid and fatal.
- Neurological symptoms necessitate testing of cerebrospinal fluid (CSF) for viral RNA.
- CSF RT-PCR may remain positive even when blood samples are negative, particularly in advanced disease.
- Neuroinflammation may be reflected by elevated CSF protein levels and mild pleocytosis.
Respiratory Tract Involvement
In addition to neurological disease, Nipah virus can cause significant respiratory pathology. Infection of respiratory epithelial cells leads to:
- Interstitial pneumonia
- Alveolar damage
- Pulmonary edema
Severe respiratory involvement is associated with higher viral loads and increased transmissibility, particularly in outbreaks characterized by human-to-human spread.
- Lower respiratory tract specimens may yield higher viral loads in severe respiratory disease.
- Persistent viral shedding in respiratory secretions underscores the importance of repeat testing in hospitalized patients.
Immune Evasion and Dysregulation
Nipah virus employs multiple mechanisms to evade and suppress host immune responses. Non-structural proteins encoded by the P gene interfere with interferon signaling pathways by inhibiting STAT-1 activation and downstream antiviral gene expression.
This immune suppression leads to:
- Delayed or reduced antibody production
- Prolonged viral replication
- Increased disease severity
Diagnostic implication
- Serological assays may be negative during early or severe infection.
- Molecular detection remains essential during the acute phase.
- Delayed seroconversion complicates retrospective diagnosis in fatal cases.
Relapsing and Late-Onset Encephalitis
A unique and clinically significant aspect of Nipah virus pathogenesis is the occurrence of relapsing or late-onset encephalitis, which may develop weeks to months after apparent recovery from the initial illness.
This phenomenon is thought to result from:
- Viral persistence in immune-privileged sites
- Incomplete immune clearance
Diagnostic implication
- Viral RNA may not be detectable in blood during relapse.
- Diagnosis often relies on CSF testing and serological evidence of prior infection.
- Long-term follow-up and documentation are critical for accurate case classification.
Laboratory Diagnosis of Nipah Virus
Laboratory diagnosis of Nipah virus infection is the cornerstone of case confirmation, patient management, and outbreak control. Due to the nonspecific nature of early clinical manifestations and the virus’s high mortality rate, rapid, accurate, and biosafe laboratory testing is essential. From a clinical laboratory perspective, diagnostic strategies for Nipah virus must balance analytical sensitivity, specificity, biosafety requirements, and turnaround time, particularly during outbreak situations.
The diagnostic approach to Nipah virus relies on a combination of molecular, serological, and confirmatory methods, selected based on the stage of illness, specimen availability, and laboratory containment capacity.
Biosafety and Containment Requirements
Nipah virus is classified as a Risk Group 4 pathogen, reflecting its high lethality, potential for human-to-human transmission, and absence of approved therapeutics. Consequently, laboratory diagnosis requires strict adherence to biosafety protocols.
- Virus isolation and propagation must be conducted exclusively in Biosafety Level 4 (BSL-4) laboratories.
- Routine diagnostic testing, including RT-PCR and serological assays, may be performed in enhanced BSL-2 or BSL-3 laboratories following validated specimen inactivation procedures.
- Personnel must be trained in handling high-consequence pathogens and use appropriate personal protective equipment (PPE).
Specimen Selection and Collection
Accurate diagnosis begins with proper specimen selection, collection, and handling. The choice of specimen depends on the clinical presentation and stage of infection.
| Specimen Type | Diagnostic Significance |
| Throat or nasopharyngeal swabs | Early detection during respiratory phase |
| Blood (serum or plasma) | Detection of viremia and serological testing |
| Cerebrospinal fluid (CSF) | Neurological involvement and encephalitis |
| Urine | Detection of prolonged viral shedding |
Specimens should be collected using sterile techniques, placed in appropriate transport media, and maintained under cold-chain conditions to preserve viral RNA integrity.
Principles of Molecular Diagnosis
Molecular detection of Nipah virus RNA is the preferred method for early diagnosis. Real-time reverse transcription polymerase chain reaction (RT-PCR) assays target conserved regions of the viral genome and allow sensitive and specific detection of viral RNA before the host mounts an antibody response.
Target Selection
- The N gene is commonly targeted due to high transcript abundance.
- The P and L genes may be included in confirmatory or multiplex assays.
- Multiple targets improve diagnostic reliability and reduce false-negative results.
Real-Time RT-PCR: Standard Diagnostic Protocol
Principle
RT-PCR involves the reverse transcription of viral RNA into complementary DNA (cDNA), followed by amplification using sequence-specific primers and fluorescent probes. The accumulation of fluorescence during amplification allows real-time detection and semi-quantitative analysis.
Step-by-Step Laboratory Workflow
- Specimen receipt and verification
- Chemical or thermal inactivation to reduce infectivity
- RNA extraction using silica column or magnetic bead-based systems
- One-step RT-PCR amplification
- Analysis of cycle threshold (Ct) values
Lower Ct values indicate higher viral RNA loads and are often associated with severe disease.
Advantages of RT-PCR
- High analytical sensitivity and specificity
- Early detection prior to seroconversion
- Ability to monitor viral load trends
Limitations
- Requires specialized instrumentation and trained personnel
- RNA degradation can lead to false-negative results
- Very early or late sampling may reduce detection sensitivity
Serological Diagnostic Methods
Serological assays are used to detect antibodies against Nipah virus and are particularly useful during the convalescent phase or for epidemiological investigations.
Enzyme-Linked Immunosorbent Assay (ELISA)
ELISA assays detect virus-specific immunoglobulins:
- IgM antibodies indicate recent or ongoing infection
- IgG antibodies reflect past exposure or recovery
ELISA assays commonly use the G or N proteins as antigens, depending on assay design.
Laboratory application
- Supports diagnosis when molecular testing is negative in late disease
- Useful for serosurveillance and outbreak investigations
Advanced Serological Platforms: AlphaLISA
AlphaLISA is a bead-based, homogeneous luminescent immunoassay that has emerged as a highly sensitive alternative to conventional ELISA.
Key features include:
- Wash-free assay format
- Reduced hands-on time
- High analytical sensitivity and specificity
- Suitability for high-throughput testing
AlphaLISA assays targeting the Nipah virus G protein have demonstrated excellent performance in detecting virus-specific antibodies.
Virus Isolation and Genomic Sequencing
Virus isolation remains the definitive method for confirming active Nipah virus infection but is restricted to specialized BSL-4 laboratories due to biosafety concerns.
Genomic sequencing provides critical insights into:
- Viral evolution
- Transmission dynamics
- Outbreak source tracing
While not used routinely, sequencing plays an essential role in public health surveillance and research.
Diagnostic Algorithm for Suspected Nipah Virus Infection
Stepwise approach:
- Clinical suspicion with epidemiological exposure
- Collection of appropriate specimens
- RT-PCR testing for viral RNA
- Serological testing if RT-PCR is negative or disease is prolonged
- Confirmatory testing and sequencing in reference laboratories
This algorithm ensures timely diagnosis while minimizing biosafety risks.
Interpretation of Laboratory Results
Molecular Results
- RT-PCR positive: Confirms acute Nipah virus infection
- High Ct value: Suggests low viral load or late infection
- RT-PCR negative with strong clinical suspicion: Repeat testing recommended
Serological Results
- IgM positive: Recent infection
- IgG positive: Past exposure or recovery
- Both negative: Early infection or alternative diagnosis
Laboratory results must always be interpreted in conjunction with clinical and epidemiological data.
Diagnostic Challenges and Limitations
- Limited availability of high-containment laboratories
- Delayed sample collection
- Inconsistent antibody responses in severe cases
- Potential cross-reactivity in serological assays
Biochemical Findings and Changes in Laboratory Diagnosis of Nipah Virus (NiV)
Acute Infection
- Thrombocytopenia and Coagulopathy: NiV infection often results in thrombocytopenia, which is attributed to endothelial damage and microvascular thrombosis.
- Elevated Inflammatory Markers: Elevated C-reactive protein (CRP) and pro-inflammatory cytokines are often observed, reflecting systemic inflammation and endothelial damage.
- Liver Dysfunction: Elevated liver enzymes (AST, ALT) are often present due to systemic endothelial injury affecting multiple organs, including the liver.
Biochemical Indicators in Disease Monitoring
- Viral Load and Disease Severity: Higher viral loads, indicated by lower cycle threshold (Ct) values, are correlated with more severe clinical outcomes.
- Delayed Seroconversion: In severe or fatal cases, there may be a delayed immune response, reflected by absent or low antibody titers during the acute phase.
Advances in Diagnostic Methods
- Enhanced Sensitivity and Specificity of RT-PCR: Advances in RT-PCR assays targeting conserved regions of the viral genome have improved early detection.
- Next-Generation Sequencing (NGS): NGS provides crucial insights into viral evolution and helps with genomic surveillance.
- Serological Assays and New Platforms: New diagnostic platforms, such as AlphaLISA, provide higher sensitivity, particularly for asymptomatic or convalescent cases.
Limitations and Precautions in Nipah Virus Diagnostics
Laboratory diagnosis of Nipah virus (NiV) is essential for effective patient management and outbreak control. However, the diagnostic process is complicated by various pre-analytical, analytical, and post-analytical challenges, each of which can affect the accuracy and clinical interpretation of test results.
Pre-Analytical Limitations:
- Specimen Selection and Timing: Early-stage infection, before significant antibody responses are detected, presents a key challenge. Real-time RT-PCR is highly effective in detecting viral RNA but its sensitivity can be compromised if the sample is collected during a period of low viral load. Early detection relies on prompt collection of high-quality specimens, such as throat or nasopharyngeal swabs, but delays or improper specimen handling can lead to RNA degradation and inaccurate results.
- Low Viral Load in Early or Late Stages: NiV infection often exhibits low viral loads in early or late stages, especially in asymptomatic or mild cases, resulting in false-negative results in RT-PCR assays. This limitation is particularly evident when specimens are obtained outside the optimal window for viral detection.
Analytical Limitations:
- Complexity of Molecular Testing: While RT-PCR is the gold standard, it requires specialized equipment and trained personnel. The sensitivity and specificity of the assay can be influenced by factors such as sample quality, RNA extraction efficiency, and viral load. Furthermore, certain molecular tests, such as multiplex assays or isothermal amplification methods, though promising, are still under development and not widely available.
- Serological Testing Limitations: Serological assays, such as ELISA and lateral flow assays, are used to detect IgM and IgG antibodies. However, these assays are limited by delayed immune responses, particularly in severe cases where antibody production is slow or impaired. In addition, serological tests can suffer from cross-reactivity with other henipaviruses, reducing their reliability in areas where these viruses are endemic.
Post-Analytical Limitations:
- Interpretation of Results: A critical issue is the misinterpretation of RT-PCR results, particularly with high Cycle Threshold (Ct) values, which could be wrongly interpreted as negative in cases with low viral loads. Additionally, clinical and epidemiological data must be correlated accurately with laboratory findings to avoid underdiagnosis or delays in confirmation, especially in areas with limited access to healthcare.
Precautions and Biosafety:
Due to the high pathogenicity and zoonotic potential of NiV, strict biosafety measures are necessary:
- Biosafety Level 4 (BSL-4) Requirements: NiV is classified as a Risk Group 4 pathogen, meaning that all diagnostic testing and virus handling must occur in BSL-4 containment facilities. Personnel must wear full PPE, including respirators, gowns, gloves, and face shields, to prevent accidental exposure.
- Sample Inactivation: Inactivation protocols must be used to ensure that viral samples do not pose a risk during transport or processing. This includes inactivating specimens before handling to avoid exposure during diagnostic procedures.
Clinical Management and Laboratory-Guided Patient Care in Nipah Virus Infection
The clinical management of Nipah virus (NiV) infection requires a multidisciplinary approach, where early laboratory diagnosis plays a crucial role in patient isolation, treatment decisions, and public health response. With no approved antiviral therapies or vaccines, management is primarily supportive, focusing on symptom relief and critical care.
Early Diagnosis and Isolation:
- Early Confirmation: Laboratory diagnosis is essential to confirm the presence of NiV and guide early clinical decisions, including the initiation of isolation protocols. Early identification not only helps in containing the virus but also ensures appropriate isolation of patients, thereby preventing nosocomial transmission.
- Infection Control: Due to human-to-human transmission, especially through respiratory secretions, strict infection control measures are required. This includes the use of personal protective equipment (PPE) by healthcare workers and isolation of confirmed and suspected cases in high-containment facilities.
Supportive Therapy:
Since no specific antiviral treatment exists, supportive care is required:
- Neurological Support: Patients with severe encephalitis require neurological monitoring, seizure control, and management of intracranial pressure (ICP) to prevent neurological deterioration.
- Respiratory Support: Severe cases may present with respiratory distress, necessitating mechanical ventilation or oxygen supplementation. Close monitoring for acute respiratory distress syndrome (ARDS) and pulmonary edema is essential.
- Symptomatic Care: Other treatments focus on managing fever, pain, and general discomfort, while ensuring that fluid balance and electrolyte levels are maintained.
Role of Laboratory Testing in Management:
- Molecular Testing for Monitoring Disease: RT-PCR testing remains crucial not only for initial diagnosis but also for monitoring viral load throughout the infection. Serial testing helps gauge the severity of the disease and inform decisions on the duration of patient isolation.
- Hematological and Biochemical Monitoring: Regular testing for thrombocytopenia and elevated inflammatory markers helps assess the extent of endothelial damage and organ dysfunction, which are key indicators of disease progression.
Public Health Role:
- Epidemiological Surveillance: Laboratory data support public health interventions such as contact tracing, risk stratification, and monitoring of transmission patterns during outbreaks. This allows for more targeted quarantine measures and helps identify potential clusters of subclinical or asymptomatic cases.
- Guiding Outbreak Management: Laboratory findings help guide outbreak response, ensuring that control measures are appropriate for the scale of the outbreak. They also contribute to the development of control strategies, including the allocation of resources for surveillance and the identification of at-risk populations.
Conclusion
Nipah virus (NiV) remains a major global health threat due to its high case fatality rate, human-to-human transmission, and its capacity to cause severe neurological and respiratory disease. Effective early diagnosis and timely patient management are essential to improve clinical outcomes and prevent outbreak spread. While RT-PCR and serological testing have significantly enhanced the capacity for accurate detection, diagnostic challenges persist due to biosafety constraints and limitations in sensitivity during early or late infection stages.
The clinical management of NiV infection continues to rely on supportive care as there are no licensed antivirals or vaccines. Laboratory data remain integral not only for diagnosis but also for disease monitoring and public health interventions. Close collaboration between clinicians, laboratory professionals, and public health authorities is crucial in outbreak management and preparedness. Strengthening diagnostic capabilities and expanding access to validated assays will be critical in mitigating the impact of future outbreaks and improving patient outcomes.
Frequently Asked Questions
References:
- Aljufri, M. I., & Mehmood, Z. (2025). A comprehensive overview of Nipah virus infection and its laboratory diagnosis. Applied Microbiology and Biotechnology. https://doi.org/10.1007/s00253-025-13474-6
- Khan, S. I., & Al-Mashoor, M. (2025). Diagnostic challenges and laboratory methods for detecting Nipah virus infections: A review. Diagnostic Microbiology and Infectious Disease, 91(1), 117101. https://doi.org/10.1016/j.diagmicrobio.2025.117101
- Jain, S., & Khan, S. A. (2025). Viral pathogenesis and therapeutic management of Nipah virus infection. Viruses, 17(6), 748. https://doi.org/10.3390/v17060748
- Bhattacharya, P., & Mollah, M. (2025). Recent developments in the study of Nipah virus infection and its impact on public health. Nature Communications, 14(1), 57219. https://doi.org/10.1038/s41467-025-57219-5
- Subramanian, K., & Pillai, A. K. (2024). Clinical management of Nipah virus: Current approaches and future perspectives. Journal of Clinical Microbiology and Infectious Diseases, 36(3), 1078. https://doi.org/10.1007/s11684-024-1078-2